Downloaded 2,053 times



































![Hyponatremic dehydration:
The pathogenesis of hyponatremic dehydration is usually due to a combination of
sodium and water loss and water retention to compensate for the volume depletion.
Occurs in children who have diarrhea and consume a hypotonic fluid (water or
diluted formula).
The initial goal in treating hyponatremia is correction of intravascular volume
depletion with isotonic fluid (NS or Ringer lactate).
The following formula can be used to calculate a patient's sodium deficit:
where [Na+]d = desired sodium concentration, [Na+]i = initial sodium
concentration, and Wt = weight in kilograms.](https://image.slidesharecdn.com/fluidtherapyinpaediatrics-140405055523-phpapp02/75/Fluid-therapy-in-paediatrics-43-2048.jpg)


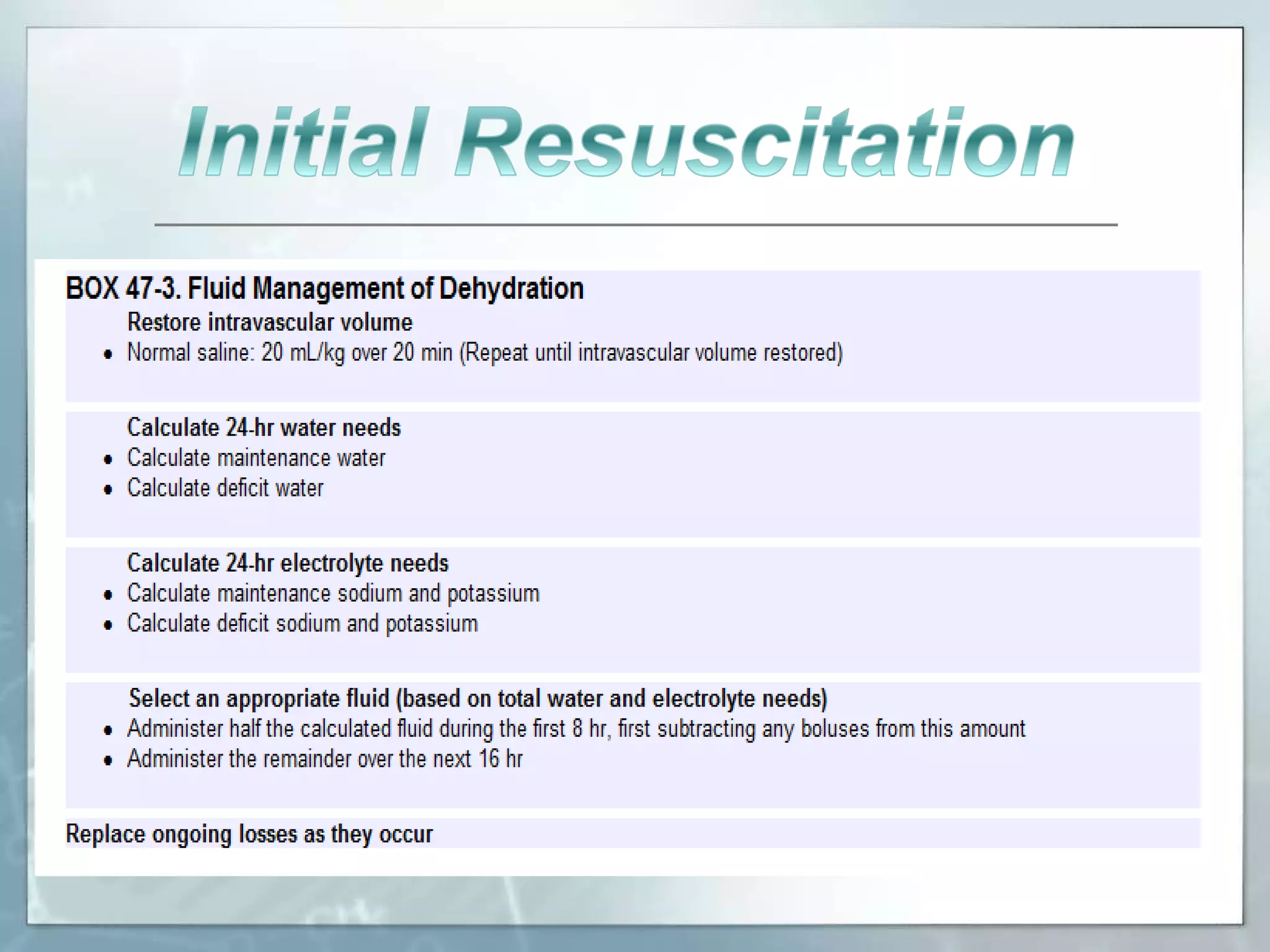
![Management
Restore intravascular volume
Normal saline: 20 mL/kg over 20 min (Repeat until intravascular volume restored)
Determine the time for correction based on the initial sodium concentration
[Na]: 145-157 mEq/L: 24 hr
[Na]: 158-170 mEq/L: 48 hr
[Na]: 171-183 mEq/L: 72 hr
[Na]: 184-196 mEq/L: 84 hr
Administer fluid at a constant rate over the time for correction
Typical fluids: D5 1/4 NS or D5 1/2 NS (both with 20 mEq/L KCl unless
contraindicated)
Typical rate: 1.25-1.5 times maintenance
Increase sodium concentration of intravenous fluid, or
Decrease rate of intravenous fluid
Decrease sodium concentration of intravenous fluid, or
Increase rate of intravenous fluid](https://image.slidesharecdn.com/fluidtherapyinpaediatrics-140405055523-phpapp02/75/Fluid-therapy-in-paediatrics-46-2048.jpg)



This document discusses fluid therapy in pediatrics. It begins by describing the composition of body fluids, including total body water and the fluid compartments. It then discusses fluid therapy, including types such as oral rehydration solution and intravenous fluids. It provides details on oral rehydration solutions, including glucose-based and cereal-based solutions. It also discusses intravenous fluid therapy and the types of crystalloid and colloid solutions. The document concludes by covering principles of fluid therapy such as maintenance and replacement therapy.



































































