![5
Imaging: From Nano to Macro - Proceedings, vol. 2006, pp. 97-100, 2006.
[6] http://www.med.nus.edu.sg/paed/resources/cardiac_thumbnail/
Table 1. Ejection Fraction by Slotted disk method, Ellipsoid investigations/echo.htm
method and provided by Phillips [7] http://www.vhlab.umn.edu/atlas/echotutorial/echotutorial1.shtml
Method Slotted Disk Ellipsoid Original [8] http://rwjms1.umdnj.edu/shindler/imageproc.html#edgefin3.m
EF(Phillips)
Ejection 55.1% 61.45% 54%
fraction
The End Systolic Volume and End Diastolic value was
calculated by calculating the pixels in the image. The pixels
along one axis give the dimension of the left ventricle along
that axis. For e.g to calculate the disk diameter the pixels
along the x axis were calculated. The number of disks was
chosen to be 20.
VII. CONCLUSION
The ejection fraction calculated using the two methods is
around 54% which is the EF measured by the Phillips
Ultrasound (Data imprinted on the image). There are still
some discrepancies in the code and the image. The apical 2
chamber view would have been a better choice for the
estimation of the volume of LV volume. This is because the
ROI is the left ventricle. The repeatability is poor as the final
result depends much on the cropping of the image to get the
ROI as the left ventricle. There are some problems regarding
the cropping the image to the ROI. If the cropping border
touches the left ventricular edge, the estimation goes wrong.
This is because the ROI is not evaluated precisely due to
opening in the region. There are several discontinuities (black
subregions) present in the filtered image. These subregions
need to be removed to get an accurate EF measurement. A
better filtering approach may remove the discontinuities.
ACKNOWLEDGMENT
I am thankful to Dr. Lobodzinsky for conducting the course
of Digital Image Processing which helped me to base my
study in the project. Further I would like to thank Dr. David
Hull and Tibor Duliskovich from Phillips Radiology
department to provide assistance in providing the images for
the project.
REFERENCES
[1] Arthur J. Vander, “Cardiovascular Physiology,” Human Physiology: Th e
Mechanisms of Body Function, 9th edition: MGH, pp 375-399, 2004
[2] Bonita Anderson, “Two dimensional echocardiographic measurements
and calculations,” Echocardiography: The Normal Examination and
Echocardiographic Measurements: Wiley, pp 96- 103, 2002
[3] T. L. Szabo, "Improving ejection fraction estimation for 2d ultrasound
using a computer-generated cardiac model," Proceedings - IEEE Ultrasonics
Symposium, pp. 1757-1760, 2008.
[4] U. Barcaro, "Automatic computation of left ventricle ejection fraction
from dynamic ultrasound images," Pattern Recognition and Image Analysis, vol.
18, pp. 351-358, 2008.
[5] M. Jolly, "Assisted ejection fraction in B-mode and contrast
echocardiography," 2006 3rd IEEE International Symposium on Biomedical](https://image.slidesharecdn.com/automatedejectionfractioncalculationsfrombmode2dechocardiographypaper-12927296100703-phpapp01/75/Ejection-Fraction-2-D-Echocardiography-5-2048.jpg)

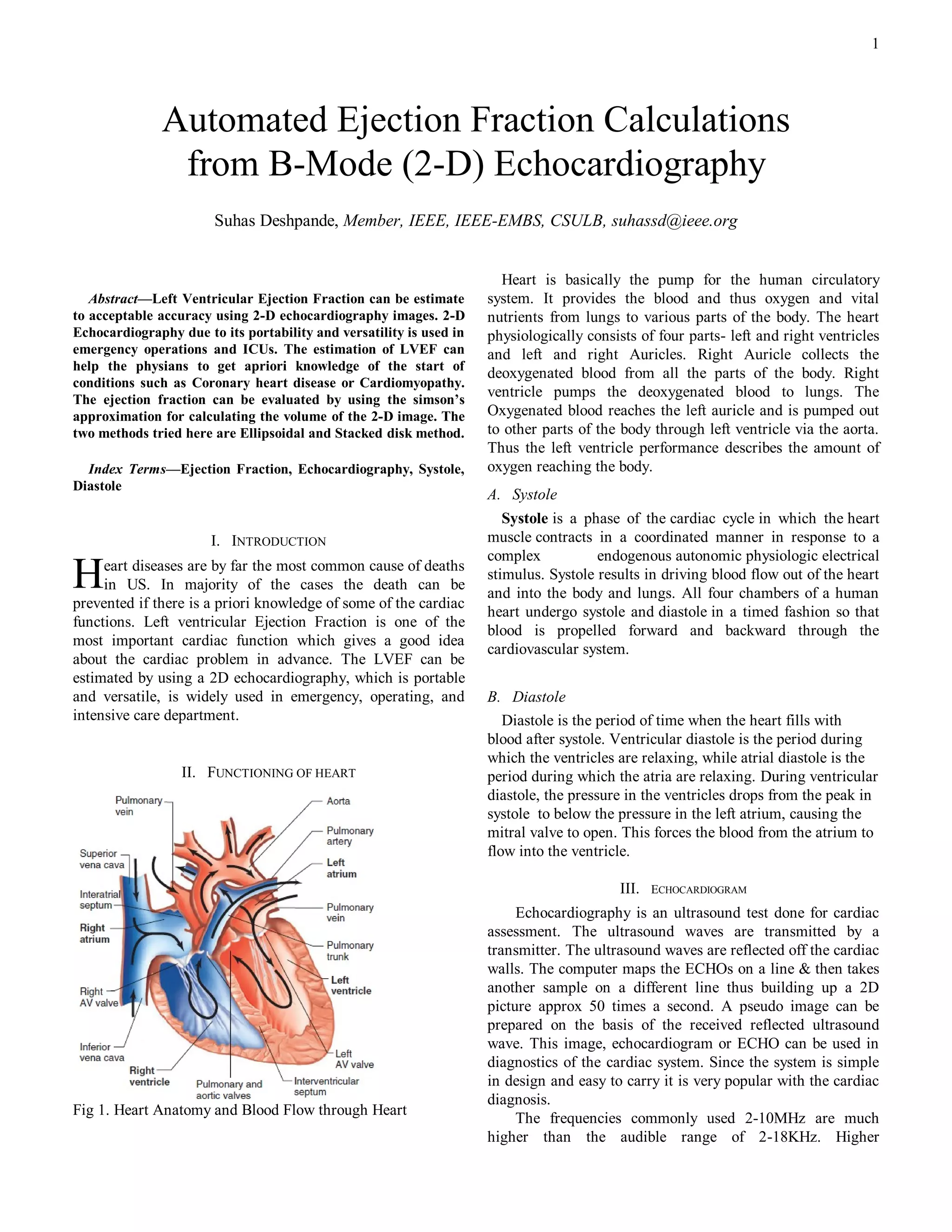
The document discusses automated calculations of left ventricular ejection fraction (LVEF) using 2-D echocardiography images, highlighting its accuracy, methodologies (ellipsoidal and stacked disk), and applications in clinical settings. It explains the cardiac cycle phases (systole and diastole) and the importance of LVEF as a key indicator of cardiac health. Additionally, it covers image analysis techniques for accurate volume estimation and the significance of echocardiography in assessing cardiac function.











































































