The document provides information on the anatomy and physiology of the human heart. It discusses the heart's location in the thoracic cavity, its internal and external structures, the layers of the heart wall, the heart chambers and valves, coronary blood supply, cardiac cycle and conduction system, heart sounds, electrocardiography, and cardiac output. The heart is described as a hollow muscular organ that pumps blood through the circulatory system through coordinated electrical conduction and mechanical contraction and relaxation of its chambers.
This presentation is an overview of the description of the 4 stages of the cardiac cycle (atrial diastole, atrial systole, ventricular systole, ventricular diastole) as well as explaining the mechanism of the cardiac cycle.
IT IS USEFULL FOR THE PHARM D & B.PHARM STUDENTS AND ALSO DIPLOMA IN PHARMACY STUDENTS AND MEDICAL STUDENTS LIKE MBBS AND DENTAL AND BHMS STUDENTSAND ALSO NUSRING STUDENTS
Be the first to comment
Anatomy And Physiology of Human Heart
1. ANATOMY OF THE HEART By: Dr Mohammed Faez
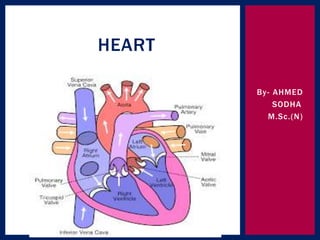
2. The Heart The heart is a chambered muscular organ that pumps blood received from the veins into the arteries, thereby maintaining the flow of blood through the entire circulatory system.
3. The Heart • The heart is surrounded by membrane called Pericardium.
4. The Pericardium • The pericardium is a fibroserous sac that encloses the heart and the roots of the great vessels. • The pericardium lies within the middle mediastinum.
5. The Pericardium
6. The Pericardium • Its function is to restrict excessive movements of the heart as a whole and to serve as a lubricated container in which the different parts of the heart can contract.
This presentation is an overview of the description of the 4 stages of the cardiac cycle (atrial diastole, atrial systole, ventricular systole, ventricular diastole) as well as explaining the mechanism of the cardiac cycle.
IT IS USEFULL FOR THE PHARM D & B.PHARM STUDENTS AND ALSO DIPLOMA IN PHARMACY STUDENTS AND MEDICAL STUDENTS LIKE MBBS AND DENTAL AND BHMS STUDENTSAND ALSO NUSRING STUDENTS
Be the first to comment
Anatomy And Physiology of Human Heart
1. ANATOMY OF THE HEART By: Dr Mohammed Faez
2. The Heart The heart is a chambered muscular organ that pumps blood received from the veins into the arteries, thereby maintaining the flow of blood through the entire circulatory system.
3. The Heart • The heart is surrounded by membrane called Pericardium.
4. The Pericardium • The pericardium is a fibroserous sac that encloses the heart and the roots of the great vessels. • The pericardium lies within the middle mediastinum.
5. The Pericardium
6. The Pericardium • Its function is to restrict excessive movements of the heart as a whole and to serve as a lubricated container in which the different parts of the heart can contract.
Location and orientation with the thorax
Structure of the heart
Structure of the Heart Wall
Chambers of the Heart
Valves of the Heart
Pathway of blood through the heart
Cardiac Muscle Tissue
Conducting System and Innervation
Four Steps of Cardiac Conduction
Blood Supply to the Heart
Cardiovascular System, Heart, Blood Vessel, ECG, Hypertension, Arrhythmia Audumbar Mali
Cardiovascular System,
Human Anatomy and Physiology-I,
The Blood Vessels,
The Heart,
The Electrocardiogram,
The Vascular Pathways,
As per PCI syllabus,
Atherosclerosis,
Coronary bypass operation,
Heart Transplants and Artificial Hearts
Health Assessment / Physical assessment.pptxsodha ranbir
It is useful for GNM-I year, B.Sc.N. Sem.-I,II students. This PPT contains Physical Assessment / Head To Toe Assessment topic of Fundamentals of Nursing subject.
This content is useful for paramedical students of GNM, & B.Sc. (N). This PPT Contain topic of Congenital Heart Disease. If you like this content kindly share this PPT to other students also.
GNC FIRST YEAR GNM OLD EXAMINATION PAPER.pdfsodha ranbir
This pdf contents some old GNC question papers of GNM-1 year.
This will helpful for only GNM-1 year students. Share this maximum to GNM-1 year students studying in Gujarat.
This content is useful for only GNM-1 year students.
This content is prepared as per INC syllabus of GNM course for first year GNM. This content cover all points of Unit-2 in microbiology syllabus well & easy to understand for first year students. This is so well-researched and thorough content. This ppt make your study of microbiology effortless. Kindly share this content more to first year GNM students.
This content is useful for only GNM-1 year students.
This content is prepared as per INC syllabus of GNM course for first year GNM. This content cover all introductory points well & easy to understand for first year students. Kindly share this content more to first year GNM students.
This content will be useful for the students of B.Sc.(N). Semester-III.
As per new revised syllabus of INC this ppt cover up Unit-I of hospital acquired infection.
Anatomy & Physiology of Renal System.pptxsodha ranbir
This content is helpful for first year students of GNM & B.Sc.(N).
This content provides you easy learning of anatomy & physiology of renal system / excretory system.
A brief information about the SCOP protein database used in bioinformatics.
The Structural Classification of Proteins (SCOP) database is a comprehensive and authoritative resource for the structural and evolutionary relationships of proteins. It provides a detailed and curated classification of protein structures, grouping them into families, superfamilies, and folds based on their structural and sequence similarities.
(May 29th, 2024) Advancements in Intravital Microscopy- Insights for Preclini...Scintica Instrumentation
Intravital microscopy (IVM) is a powerful tool utilized to study cellular behavior over time and space in vivo. Much of our understanding of cell biology has been accomplished using various in vitro and ex vivo methods; however, these studies do not necessarily reflect the natural dynamics of biological processes. Unlike traditional cell culture or fixed tissue imaging, IVM allows for the ultra-fast high-resolution imaging of cellular processes over time and space and were studied in its natural environment. Real-time visualization of biological processes in the context of an intact organism helps maintain physiological relevance and provide insights into the progression of disease, response to treatments or developmental processes.
In this webinar we give an overview of advanced applications of the IVM system in preclinical research. IVIM technology is a provider of all-in-one intravital microscopy systems and solutions optimized for in vivo imaging of live animal models at sub-micron resolution. The system’s unique features and user-friendly software enables researchers to probe fast dynamic biological processes such as immune cell tracking, cell-cell interaction as well as vascularization and tumor metastasis with exceptional detail. This webinar will also give an overview of IVM being utilized in drug development, offering a view into the intricate interaction between drugs/nanoparticles and tissues in vivo and allows for the evaluation of therapeutic intervention in a variety of tissues and organs. This interdisciplinary collaboration continues to drive the advancements of novel therapeutic strategies.
Slide 1: Title Slide
Extrachromosomal Inheritance
Slide 2: Introduction to Extrachromosomal Inheritance
Definition: Extrachromosomal inheritance refers to the transmission of genetic material that is not found within the nucleus.
Key Components: Involves genes located in mitochondria, chloroplasts, and plasmids.
Slide 3: Mitochondrial Inheritance
Mitochondria: Organelles responsible for energy production.
Mitochondrial DNA (mtDNA): Circular DNA molecule found in mitochondria.
Inheritance Pattern: Maternally inherited, meaning it is passed from mothers to all their offspring.
Diseases: Examples include Leber’s hereditary optic neuropathy (LHON) and mitochondrial myopathy.
Slide 4: Chloroplast Inheritance
Chloroplasts: Organelles responsible for photosynthesis in plants.
Chloroplast DNA (cpDNA): Circular DNA molecule found in chloroplasts.
Inheritance Pattern: Often maternally inherited in most plants, but can vary in some species.
Examples: Variegation in plants, where leaf color patterns are determined by chloroplast DNA.
Slide 5: Plasmid Inheritance
Plasmids: Small, circular DNA molecules found in bacteria and some eukaryotes.
Features: Can carry antibiotic resistance genes and can be transferred between cells through processes like conjugation.
Significance: Important in biotechnology for gene cloning and genetic engineering.
Slide 6: Mechanisms of Extrachromosomal Inheritance
Non-Mendelian Patterns: Do not follow Mendel’s laws of inheritance.
Cytoplasmic Segregation: During cell division, organelles like mitochondria and chloroplasts are randomly distributed to daughter cells.
Heteroplasmy: Presence of more than one type of organellar genome within a cell, leading to variation in expression.
Slide 7: Examples of Extrachromosomal Inheritance
Four O’clock Plant (Mirabilis jalapa): Shows variegated leaves due to different cpDNA in leaf cells.
Petite Mutants in Yeast: Result from mutations in mitochondrial DNA affecting respiration.
Slide 8: Importance of Extrachromosomal Inheritance
Evolution: Provides insight into the evolution of eukaryotic cells.
Medicine: Understanding mitochondrial inheritance helps in diagnosing and treating mitochondrial diseases.
Agriculture: Chloroplast inheritance can be used in plant breeding and genetic modification.
Slide 9: Recent Research and Advances
Gene Editing: Techniques like CRISPR-Cas9 are being used to edit mitochondrial and chloroplast DNA.
Therapies: Development of mitochondrial replacement therapy (MRT) for preventing mitochondrial diseases.
Slide 10: Conclusion
Summary: Extrachromosomal inheritance involves the transmission of genetic material outside the nucleus and plays a crucial role in genetics, medicine, and biotechnology.
Future Directions: Continued research and technological advancements hold promise for new treatments and applications.
Slide 11: Questions and Discussion
Invite Audience: Open the floor for any questions or further discussion on the topic.
What is greenhouse gasses and how many gasses are there to affect the Earth.moosaasad1975
What are greenhouse gasses how they affect the earth and its environment what is the future of the environment and earth how the weather and the climate effects.
This presentation explores a brief idea about the structural and functional attributes of nucleotides, the structure and function of genetic materials along with the impact of UV rays and pH upon them.
Cancer cell metabolism: special Reference to Lactate PathwayAADYARAJPANDEY1
Normal Cell Metabolism:
Cellular respiration describes the series of steps that cells use to break down sugar and other chemicals to get the energy we need to function.
Energy is stored in the bonds of glucose and when glucose is broken down, much of that energy is released.
Cell utilize energy in the form of ATP.
The first step of respiration is called glycolysis. In a series of steps, glycolysis breaks glucose into two smaller molecules - a chemical called pyruvate. A small amount of ATP is formed during this process.
Most healthy cells continue the breakdown in a second process, called the Kreb's cycle. The Kreb's cycle allows cells to “burn” the pyruvates made in glycolysis to get more ATP.
The last step in the breakdown of glucose is called oxidative phosphorylation (Ox-Phos).
It takes place in specialized cell structures called mitochondria. This process produces a large amount of ATP. Importantly, cells need oxygen to complete oxidative phosphorylation.
If a cell completes only glycolysis, only 2 molecules of ATP are made per glucose. However, if the cell completes the entire respiration process (glycolysis - Kreb's - oxidative phosphorylation), about 36 molecules of ATP are created, giving it much more energy to use.
IN CANCER CELL:
Unlike healthy cells that "burn" the entire molecule of sugar to capture a large amount of energy as ATP, cancer cells are wasteful.
Cancer cells only partially break down sugar molecules. They overuse the first step of respiration, glycolysis. They frequently do not complete the second step, oxidative phosphorylation.
This results in only 2 molecules of ATP per each glucose molecule instead of the 36 or so ATPs healthy cells gain. As a result, cancer cells need to use a lot more sugar molecules to get enough energy to survive.
Unlike healthy cells that "burn" the entire molecule of sugar to capture a large amount of energy as ATP, cancer cells are wasteful.
Cancer cells only partially break down sugar molecules. They overuse the first step of respiration, glycolysis. They frequently do not complete the second step, oxidative phosphorylation.
This results in only 2 molecules of ATP per each glucose molecule instead of the 36 or so ATPs healthy cells gain. As a result, cancer cells need to use a lot more sugar molecules to get enough energy to survive.
introduction to WARBERG PHENOMENA:
WARBURG EFFECT Usually, cancer cells are highly glycolytic (glucose addiction) and take up more glucose than do normal cells from outside.
Otto Heinrich Warburg (; 8 October 1883 – 1 August 1970) In 1931 was awarded the Nobel Prize in Physiology for his "discovery of the nature and mode of action of the respiratory enzyme.
WARNBURG EFFECT : cancer cells under aerobic (well-oxygenated) conditions to metabolize glucose to lactate (aerobic glycolysis) is known as the Warburg effect. Warburg made the observation that tumor slices consume glucose and secrete lactate at a higher rate than normal tissues.
Richard's entangled aventures in wonderlandRichard Gill
Since the loophole-free Bell experiments of 2020 and the Nobel prizes in physics of 2022, critics of Bell's work have retreated to the fortress of super-determinism. Now, super-determinism is a derogatory word - it just means "determinism". Palmer, Hance and Hossenfelder argue that quantum mechanics and determinism are not incompatible, using a sophisticated mathematical construction based on a subtle thinning of allowed states and measurements in quantum mechanics, such that what is left appears to make Bell's argument fail, without altering the empirical predictions of quantum mechanics. I think however that it is a smoke screen, and the slogan "lost in math" comes to my mind. I will discuss some other recent disproofs of Bell's theorem using the language of causality based on causal graphs. Causal thinking is also central to law and justice. I will mention surprising connections to my work on serial killer nurse cases, in particular the Dutch case of Lucia de Berk and the current UK case of Lucy Letby.
2. The heart is a roughly cone shaped hollow
muscular organ.
Length: 10 cm
Weight: 225 g in women
310 g in men
Position/location: the heart lies in the thoracic
cavity in the mediastinum( the space between
two lungs).
It lies obliquely little more to the left that right
and presents a base above and apex below.
INTRODUCTION
3. Inferiorly: the apex rests on the central tendon of
the diaphragm.
Superiorly: the great blood vessels e.g. aorta,
superior venacava, pulmonary artery and
pulmonary veins
Posteriorly: the oesophagus, trachea, left and
right bronchus, descending aorta, inferior
venacava and thoracic vertebra
Laterally: the lungs- the left lungs overlaps the
left side of the heart
Anteriorly: the sternum , ribs and intercostal
muscles.
ORGANS ASSOCIATED
WITH THE HEART
4. The heart wall:
The heart wall is composed of three layers of the
tissue.
1. Pericardium
2. Myocardium
3. endocardium
STRUCTURE OF THE HEART
5.
6. The pericardium is the outermost layer of the
heart and is made up with two sacs.
Outer sac consist of : fibrous tissue
Inner sac consists of : continues double layer of
serous membrane
Outer layer is known as parietal pericardium
Inner layer is known as visceral pericardium.
the space between two sacs is known as
pericardial space, which is filled with serous
fluid, which is secreted from serous membrane of
inner sac.
1. PERICARDIUM
7. The myocardium is composed of specialised
cardiac muscles founded only in heart.
It is not under voluntary control but striated like
skeletal muscle. Each fibres cells has nucleus
and one or more braches.
The sheet arrangements of the myocardium
enables the atria and ventricular to contract in a
co ordinated and efficient manner.
Myocardium is network of specialised conducting
fibres responsible for transmitting the heart
electrical signals.
Myocardium is thickest at the apex and thins
out towards the base.
2. MYOCARDIUM
8. This lines the chambers and valves of the hearts.
It is a thin smooth membrane to ensure smooth
flow of blood through the heart. It consists of
flattened epithelial cells and it is continuous
with the endothelium lining the blood vessels.
3. ENDOCARDIUM:
9. The heart is divide into right and left sided by
the septum, a partition consisting of myocardium
converted by endocardium.
Each side is divide by an antrioventricular valve
into upper atrium and the ventricle below.
Atrioventricular valve: these are formed by
double layer of endocardium.
Strengthen by a little fibrous tissue.
INTERIOR OF THE HEART
10.
11. AV VLAVES: right side AV valve has three flaps
is known as tricuspid valve, which separates
right atrium and right ventricle.
Left sided AV valve has two flaps is called as
mitral valve or bicuspid valve, which separates
left atrium and left ventricle.
12. There are four chambers of the heart.
1. right atrium – 2- 3 mm size
2.rigth ventricle-4-5 mm
3. left atrium – 2-3 mm
Left ventricle- 10-15 mm
CHAMBERS OF THE HEART
13. The two largest veins of the body, the superior
vencava and inferior vencava empty their
contents into the right atrium.
This blood passes via right atrioventriculer vlave
into right ventricle and from there blood is
pumped out into the pulmonary artery( the only
artery in the body which caries deoxygenated
blood).
BLOOD FLOW THROUGH THE
HEART
14. At the opening of pulmonary artery pulmonary
valve is present which prevents backflow of the
blood into right ventricle , it is also known as
semi-luner valve.
After leaving the heart the pulmonary artery
divides into left and right pulmonary arteries,
which carry the blood to the lungs where
exchange of gases takes place, carbon dioxide
excreted and oxygen is absorbed.
15. After purification of blood in the lungs two
pulmonary veins carry oxygenated blood back to
the left atrium.
Blood than passes through left atrioventriculer
valve ( mitral valve, bicuspid valve) into the left
ventricle and from there blood Is pumped out into
the aorta( the first artery of general circulation).
The opening of aorta is guarded by the aortic
valve.( at the opening of aorta there are valve
present which is called as semilunar or aortic
valve.
16. However , it should be noted that both atria
contract at the same time and this followed by
the simultaneous contraction of both ventricles.
17.
18. arterial supply: the heart I supplied with arterial
blood by the right and left coronary arteries.
The coronary arteries branch from the ascending
aorta.
The coronary arteries receives about 5% of the
blood pumped from the heart.
Large amount of blood supply especially to the left
ventricle.
There are two coronary arteries :
1. Right coronary artery
2. Left coronary artery
BLOOD CIRCULATION TO THE
HEART/ CORONARY CIRCULATION
19.
20. 1. right coronary artery:
It supplies small branches to the right side heart.
Right arteries having two branches:
Posterior inter ventricular branch
Marginal branches
The posterior inter ventricular branches supplies
blood to the wall of two ventricles.
The marginal branches supplies blood to the
right ventricles.
21. 2. left coronary artery:
The left coronary artery passes inferior to the
left circle & divides into the anterior inter
ventricular branch & the circumflex branches.
The anterior inter ventriculer branches will
supplies oxygenated blood to the walls of both
ventricles.
The circumflex branch will supplies oxygenated
blood to the walls of the left ventricle & left
atrium.
22.
23. Venous drainage: most of venous blood is
collected into number of cardiac veins that join to
form the coronary sinus, which opens into the
right atrium.
24. Autorythmicity: THE heart posses the property
of generating its own electrical impulse & beats
independently of nervous or hormonal control.
It is sullied with both sympathetic & Para
sympathetic automic nerve fibres.
Components: SA NODE: sino-atrial node
AV NODE: atrio-ventricular node
AV bundle( bundle of his): atrio ventricular
bandle
CONDUCTIVE SYSTEM OF HEART
25.
26. SA NODE: SINO ATRIAL NODE
This is small mass of specialise cells lies in the opening of
the superior venacava.
The Sino atrial cells generates these regular impulses
because they are electrically unstable.
This is also known as parameters.
AV NODE: atrioventriculer node
This is small mass of neuromuscular tissue is situated in
the wall of the atrial septum near the arioventricular
valve.
Normally AV node merely transmit the electrical signals
from the atria into ventricle.
27. 3. atriovenriculaer bundle( bundle of his)
This mass of specialised fibres originated from the
AV node.
The AV node crosses the fibrous ring that separates
atria and ventricles , then at the upper end of
ventricular septum, it divides into right and left
bundle branches.
Within the ventricular myocardium the branches
break up into the fibres called parkinje fibres, which
supplies electrical impulses into the apex of the
heart.
28. Heart is influenced by the autonomic( sympathetic &
para sympathetic nerves originating in the
cardiovascular centre in the medulla oblongata.
The vegus nerve: supply mainly the SA node & AV
nodes & atrial muscles.
NERVE SUPPLY TO THE HEART
30. At rest the healthy adult heart is likely to beat at a
rate of 60-70 bpm.
Each heart beat cycle is known as cardiac cycle .
During this time heart will contract & relax.
The period of contraction is called as systole &
relaxation is called as diastole.
31. Each cardiac cycle lasts about 0.8. sec consists of :
1.Atrial systole: contraction of atria 0.1 sec
2. Ventricular systole : contraction of ventricles 0.3
secs
3. Complete cardiac diastole:
Relaxation of atria & ventricles 0.4 secs
STAGES OF CARDIAC CYCLE
32.
33. The superior venacava & inferior vencava transport deoxygenated
blood into the right atrium at the same time four pulmonary
veins bring oxygenated blood into the left atrium.
Through AV valves
Blood flows passively into left ventricle(SA node spreads a wave
of impulse into myocardium of left atrium & starts)
Atrial contraction
AV node spreads , impulses quickly into ventricular muscle via
the AV bundle & purkinje fibres
34. A wave of contraction sweeps upward from apex of the heart
across the both ventricles
Ventricular contraction
Blood pumps into pulmonary artery & aorta
After contraction of ventricles the atrium & ventricles relax
Myocardium recover in preparation for the next heartbeat &
atria refill for next cycle
35. Heart sound is a involuntary action.
There are four heart sounds. Each corresponding to a
particular event in the cardiac cycle.
LUB: first sound , fairly loud occurs due to closure of
atrioventriculer vlave.
DUP: softer , sound due to closure of aortic and
pulmonary valves.
HEART SOUND
36. It is the report of electrical activity of the heart.
The pattern of electrical activity may be displayed on
an oscilloscope screen or traced on paper.
The normal ECG showing five waves by convention ,
have been named PQ,R,S, &T.
P wave: it arise when impulse from the SA NODE
sweeps over the atria( atrial depolarisation)
The QRS wave: it represent the very rapid spread of
the impulse from the AV node through the a bundle &
the purkinjie fibres & the electrical activities of the
ventricular muscle.
ECG: ELETROCARDIOGRAM
38. T WAVE: it represents the relaxation of the ventricular
muscle.( ventricular repolarization)
The ECG described above originated from the SA NODE
and is known as sinus rhythm.
P: atrial contraction
QRS: ventricular contraction
T: ventricular relaxation
39. The cardiac output is the amount of blood ejected
from each ventricle every minute.
The amount of blood expelled by each contraction of
each ventricle is the stroke volume.
Cardiac output is expressed in litters per minutes.
Cardiac out put = stroke volume * heart beat
In healthy adult heart at rest the stroke volume is
approximately 70ml and per minute heart rate is 72
per minute
Cardiac out put will be 5 liter/ minute
CARDIAC OUTPUT
41. Blood pressure is the force pressure that the blood
exerts on the walls of the blood vessels.
Blood pressure varies according to the times of the
day, posture, gender, age of the individual.
Blood pressure= systolic pressure
diastolic pressure
Systolic pressure:
When the left ventricular contracts & pushes blood
into the aorta, the pressure produced within the
arterial system is called the systolic blood pressure.
In adult it will be 120 mm of Hg or 16 Kpa( kilo
paskal)
BLOOD PRESSURE
42. Diastolic pressure:
When complete cardiac diastole occurs & the heart
is resting following the ejection of the blood , the
pressure within the arteries is much lower & is called
diastole blood pressure. In adult it will be 80 mm of
Hg 0r 11 Kpa.
BP= 120 mm of HG/ 80 mm of Hg
Blood pressure = cardiac output * peripheral
resistance
43. blood pressure is controlled in two ways.
1. short term control:
Moment to moment basis which mainly involves
1. baroreceptor reflex
2. chemo receptor reflex
3. higher centres in the brain
2. Long term control:
it involves regulation of blood by kidney and renin
angiotensin – aldosterone system( RAAS)
CONTROL OF BLOOD PRESSURE
44. Cardio vascular centre (CVC): it is collection of
interconnected nervous in the brain & situated in the
medulla & pons.
BARORECEPTORS:
These are nerve ending sensitive to pressure
changes ( stretch) within the vessel, situated in the
arch of aorta and in the carotid sinuses.( these are
body’s principal moment to moment regulatory
mechanism for controlling blood pressure.
1. SHORT TERM BP REGULATION
45. Chemoreceptors: these are the nerve ending situated in the
carotid and aortic bodies.
1. BARORECEPTORS:
When BP increases(BP more than 120 mm of hg)
Stimulation of baroreceptors in the aorta
Sending the impulses in to the cardiovascular centre in the
brain
CVC stimulates the parasympathetic nervous system
Relaxation of muscle of blood vessels ( tunica media)
Vasodilation
Blood pressure will decrease
46. when BP decreases less than 120/80 mm of Hg
Stimulation of brain receptors in the aorta
Sending impulses into the CVC in the brain
CVC will pass message into sympathetic nervous system
Stimulation of sympathetic nerve system
Contraction of muscles of blood vessels ( tunica media)
Vasoconstriction
BP will increase
47.
48. When co2 level increases & O2 level decrease in the blood stream
Tissue hypoxia
Need to improve tissue perfusion
Blood pressure should increase in this situation,
chemoreceptor will recognize this changes in CO2 & O2 in the blood
stream.
Pass this contraction to CVC in the brain
CVC will stimulate sympathetic nerve system
Vasoconstriction
BP will increase
CHEMORECEPTORS:
49.
50. when emotional status such as fear, anxiety, pain , anger,
occurs.
Hypothalamus will get stimulated
Brain need more blood supply
It will stimulate sympathetic nerve system
Vasoconstriction
BP increases thus brain will get more blood supply,
HIGHER CENTRE IN THE BRAIN
51. RAAS: renin angiotensin – aldosterone system
It is the mechanism where involvement of kidney is possible.
When kidney is unable to get blood supply , only this mechanism
will be activated.
Low renal blood flow
Decreased blood volume
Decreased BP
Kidney will secret renin
Angiotensinogen _____ angiotensin I
ACE
LONG TERM MECHANISM
52. Angiotensin II
Adrenal cortex vasoconstriction
Secretion of aldosterone increased BP
Kidney tubules reabsorbs kidney will get adequate blood supply
Na & water
Increased blood volume
Increased BP
53. Although circulation of blood around the body is
continues. It is described into two parts.
A. pulmonary circulation
B. systemic circulation
CIRCULATION OF BLOOD
54.
55.
56. This consist of the circulation of blood from the right
ventricle of the heart to the lungs & back to the left
atrium.
The pulmonary arteries: there are two branches for the
pulmonary trunk,
1. right pulmonary artery: it passes to the root of the
right lungs & divides into the branches.
- larger branches carries blood into middle & lower lobes
- smaller branches carries into upper lobe
2. the left pulmonary artery; it runs to the left lungs
where it divides into two branches.
One passing into each lobe.
A. PULMONARY CIRCULATION
57. Within the lungs these arteries divides & subdivide into smaller
arteries,
Arterioles
Capillaries
the inter change of O2 & CO2 takes place between capillary
blood & air in the alveoli of the lungs.
After gas exchanges each capillaries will join together & forms
vessels.
Capillaries
Veinules
veins
58. there are two pulmonary veins.
Right & left pulmonary veins
This both will carry oxygenated blood into left atrium
of the heart.
59. It is the circulation of blood all around the body.
The blood pumped out from the left ventricle is
carried by the branches of the aorta around the body
& is returned to the right atrium of the heart by
superior & anterior vencava is known as systemic
circulation.
2. SYSTEMIC / GENERAL CIRCULATION
60. Blood vessels are acting as pumps to supply blood
through out the body.
Blood vessels vary in structure size, function & these
are several types
Arteries
Arterioles
Capillaries
Venules
veins
BLOOD VESSELS
61.
62.
63. These are the blood vessels that transport blood
away from the heart.
They vary in considerably in size & their wall consist
of their layers of tissue.
Tunica adventitia: outer layer : fibrous tissue
Tunica media : middle layer: smooth muscle &
elastic tissue
Tunica intima: inner layer: squamous epithelial tissue
ARTERIES & ARTERIOLES
64.
65.
66. Anastomosis are arteries that form a link between
main arteries supplying an area.
End arteries are the arteries with no anastomoses or
those beyond the most distal anastomosis.
ANASTOMOSIS & END ARTERIES
67.
68. The smallest arterioles break into a number of
minotic vessels called capillaries.
The walls consist of a single layers of endothelial
cells sitting on a very thin basement membrane.
Through which water & other small molecules can
pass.
Entry to capillaries bed is grounded by rings of
smooth muscle( pre capillary sphincters) that directs
the blood vessels.
In certain places, including liver & bone marrow, the
capillaries are significantly wider & thicker than
normal. These are known as SINUSOIDS.
CAPILLARIES & SINUSOIDS
69.
70.
71. Veins are blood vessles that returns blood at low
pressure to the heart. The walls of the veins are the
thinner than those of arteries but have the same
three layers of tissue.
Veins are having valves, which prevent backflow of
blood. These are formed by folds of tunica intima &
strengthen by connective tissue.
Smallest veins are called as venules.
VEINS & VENULES
72. The outer layer of tissue of thick walled blood
vessels receive & the their blood walled blood
supply via network of blood vessels called the vasa
vasorum.
Thin walled vessels & the endothelium of other
receives O2 & nutrients by diffusion from the blood
passing trough them.
BLOOD SUPPLY
73. Vasomotor centre in medulla oblongata
Autonomic nerve system
Sympathetic stimulation para sympathetic stimulation
Contraction of smooth relaxation of smooth muscle
tunica media muscle of tunica media
Vasoconstriction vasodilatation
Lumen of blood vessel lumen of blood vessel increase
decreased
NERVE SUPPLY
74. The aorta is biggest artery in the human body &
begins at the upper part of the left ventricle &
passing up wards for short way , it arches back
wards and to the left.
It then descends behind the heart through the
thoracic cavity a little to the left of the thoracic
vertebrae.
At the level of 12th thoracic vertebra it passes behind
the diaphragm then downwards in the abdominal
cavity to the level of 4th lumber vertebra, where it
divides into the right and left common iliac arteries.
AORTA
75. The aorta will be described here according to its
location.
1. thoracic aorta:
This is the part of aorta lies above the diaphragm
and is described in three parts.
- ascending aorta
- arch of aorta
- descending aorta in the thorax
76. A. ascending aorta:
It is about 5 cm long , lies behind the sternum.
Two blood vessels stating from ascending aorta that are, right
and left coronary artery.
77.
78. B. Arch of aorta:
The arch of aorta is continuation of ascending aorta.
It begins behind the manubrium of the sternum and runs up
wards, back wards and to the left in front of trachea.
And it is continuous with the descending aorta.
- brachiocephalic artery
-Left common carotid artery
-Left subclvian artery
79. The venous blood from head & neck is returned by deep &
superficial veins.
The superficial veins will drain blood from superficial area of
the brain & deep vein drain from deep area of deep of brain.
Veins of head and neck:
1. right and left middle temporal vein
2. right and left supra orbital veins
3. right and left maxillary vein
4. right and left facial vein
5. right and left lingual vein
6. right and left occipital veins
VENUS RETURNS FROM THE HEAD &
NECK
80.
81.
82. The greater part of the brain is supplied by
arrangement of arteries called the circle of
willis. It consist of following arteries:
Two internal carotid arteries
Two vertebral arteries
CIRCULUS ARTERIOSOS (CIRCLE OF
WILLI)
87. The veins of upper limb is divided into two groups:
1. Deep veins:
Metacarpal veins
Deep palmar venous arch
Brachial veins
Axillary veins
2. Superficial veins
Cephalic vein
Basilica veins
Median veins
Medial cubital veins
Both join together & forms subclavian veins.
VENUS SUPPLY:
88. This is the part of aorta which continuous with
arch of aorta & begins at the 4 the thoracic
vertebra & extends downwards on the anterior
surface of the thoracic vertebra.
The descending aorta in the thorax gives of many
paired branches those are,
Bronchial arteries: supply to brachia & lungs
Oesophagus arteries: oesophagus
Intercostal artery: ribs, intercostal muscles
DESCENDING AORTA:
89.
90. There are two veins to drain venous blood in
thoracic cavity.
Azygos vein & hemizygos vein
The brachial vein, oesophageal vein & intercostal
vein join together & forms these two main veins.
Azygos vein joins with superior venacva &
hemizyagose vein join with left brachiocephalic
vein.
VENOUS RETURNS:
91.
92.
93.
94. The abdominal aorta is the continuation of thoracic
aorta& entering behind diaphragm at the 12th
thoracic vertebrae , at the level of 4ht lumber
vertebrae. it will divide into two common iliac artery.
Many branches arises from the abdominal aorta.
Paired branches:
Inferior phrenic artery : diaphragm
Renal artery: kidney
Superior renal artery: adrenal gland
Testicular artery: testes
Ovarian artery: ovary
ABDOMINAL AORTA:
95. Unpaired branches:
1. The coeliac artery: is short, thick, 1.25cm long & it rises
immediate below the diaphragm 7, divides into 3 branches.
Left gastric artery: stomach
Splenic artery: pancreas & spleen
Hepatic artery: liver, gall bladder, duodenum
2. Superior mesenteric artery:
It is a branch from aorta between the coeliac artery & renal
artery & supply blood supply to small intestine & proximal
part of large intestine.
3. Inferior mesenteric artery:
It arises from aorta about 4cm above its division into common
iliac artery. It supplies distal half of large intestine & part of
rectum.
96.
97. Paired testicular, ovarian, renal & adrenal veins
join into directly inferior venacava.
Blood from remaining organs in the abdominal
cavity passes through the liver via PORTAL
CIRCULATION & enter into interior venacva.
VENUS RETURN:
98. In the portal circulation, venous blood passes
from the capillary beds of the abdominal part of
the digestive system, spleen, pancreas to the
liver.
In this way blood with a high concentration of
nutrients, absorbed from the stomach and
intestines goes to the liver first.
In liver certain modification take place including
the regulation of blood nutrients levels.
It passes in second capillary bed , the hepatic
sinusoids & from portal vein.
PORTAL CIRCULATION:
99.
100. PORTAL VEIN:
This is formed by the union of the following veins, each of
which drains blood from the area supplied by
corresponding artery.
Splenic vein: drains blood spleen , pancreas, part of
stomach
Inferior mesenteric vein: rectum, pelvic, descending colon
of large intestine.
Superior mesenteric vein: small intestine, proximal part
of large intestine
Gastric vein: stomach. Distal end of oesophagus
Cystic vein: gall bladder
101. HEPATIC VEIN:
These are very short veins that leave the
posterior surface of the liver & almost
immediately enter the inferior vencava.
102. Abdominal aorta will divide into right & left
common iliac artery. These are divided into
further two branches.
Internal iliac artery
External iliac artery
Internal iliac artery:
It will supply organs in the pelvic cavity. In
female: uterine artery
CIRCULATION OF PELVIS & LOWER LIMB:
103. External iliac artery:
It will obliquely downwards & passes into where it
divides femoral artery & branches into popliteal
artery which supply blood to the knee area and
popliteal fossa. It further divides into :
The femoral artery: begins at midpoint at the
inguinal ligament & extends downwards in front of
the thigh. Then it eventually passes through
popliteal space where it becomes the popliteal artery.
Popliteal artery: it passes through the popliteal fossa
behind the knee, where pulse can be felt. At lower
border of the popliteal fossa it divides into the
anterior and posterior tibial arteries.
104. Anterior tibial artery: which supplies blood
supply to the tibia, ankle joint. It will divide over
the dorsum of foot & forms dorsalis pedis artery.
Posterior tibial artery: it runs medially back of
legs & gives a branch peroneal artery which
supplies lateral aspect of the leg & forms a new
branch- planter artery, which supplies blood to
the sole of the foot.
106. 1. Deep veins:
Digital vein
Planter venous arch
Post tibial vein
Anterior tibial vein
Popliteal vein
Femoral vein
External iliac vein
Internal iliac vein
Common iliac vein
Both right & left common iliac veins joins into inferior
venacava at the sacro iliac joint.
VENUS RETURN:
107.
108. 2. Superficial vein: there are two main superficial
veins are draining blood from the lower limbs are,
Small saphenous vein: the small saphenous vein
begins behind the ankle joint& joins into
popliteal vein.
Great saphenous vein: it is the longest vein of
the body, it begins at the medial half of the
dorsum of the foot & runs upwards crossing over
thigh & joins into political vein.