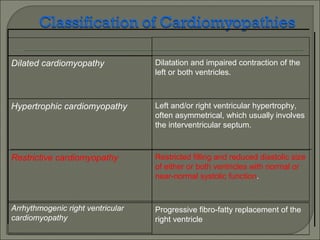
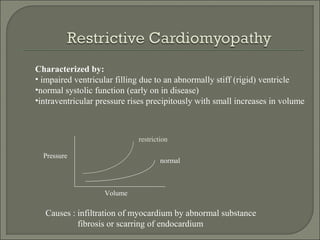
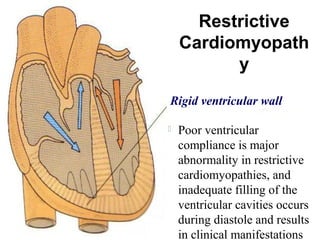
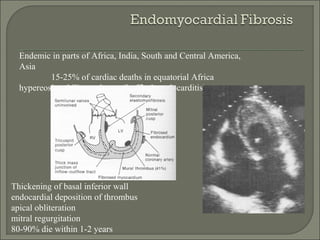
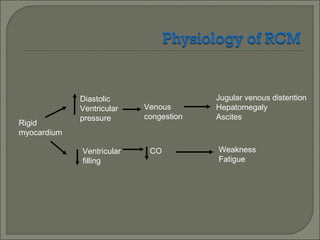
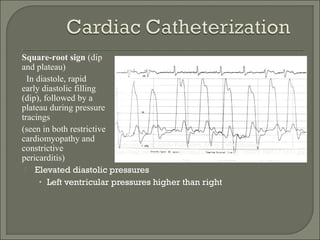
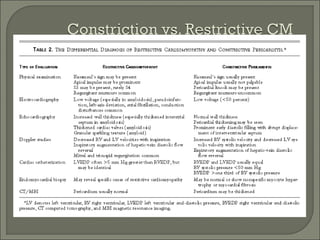
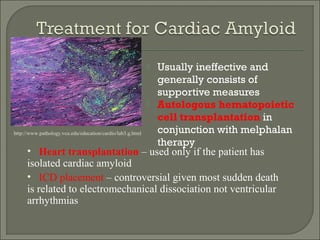
Restrictive cardiomyopathy is characterized by stiff ventricles that do not fill properly, though systolic function is usually preserved initially. It can be caused by infiltrative diseases, fibrosis, or other processes that restrict ventricular filling. On echocardiogram, restrictive cardiomyopathy shows impaired ventricular filling and enlarged atria, while cardiac catheterization reveals elevated diastolic pressures and a distinctive "square root sign" pressure tracing. Treatment focuses on managing symptoms and underlying causes if identifiable, though prognosis is often poor without transplantation.























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)



