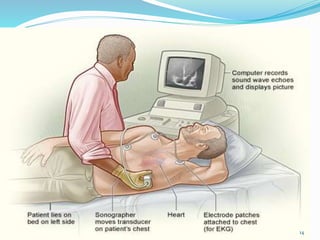
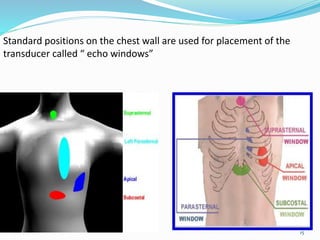
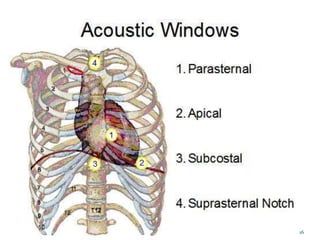
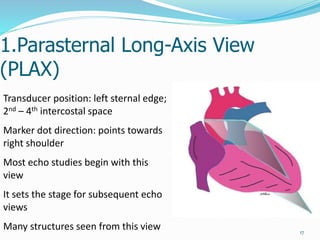
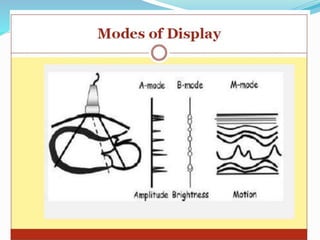
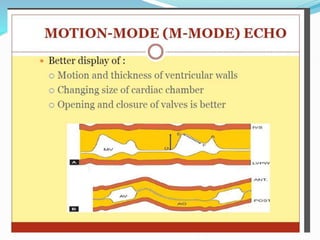
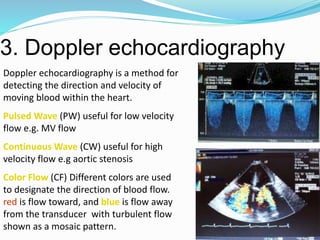
The document provides an overview of basic echocardiography. It discusses the history and development of echocardiography. It describes how ultrasound images are generated using transducers that transmit sound waves and receive echoes. Standard echocardiogram views and modalities including 2D, M-Mode, and Doppler are summarized. Indications for echocardiography including assessing valve disease, function, masses and endocarditis are covered in brief.

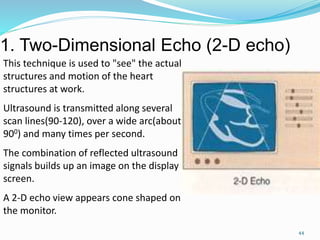














































![2._Intro_to_echo_and___instrumentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/2-250726161338-64c6d201-thumbnail.jpg?width=640&height=640&fit=bounds)






























