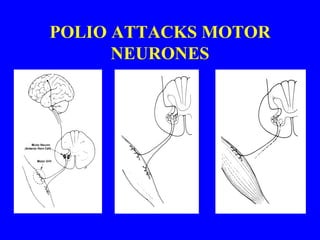
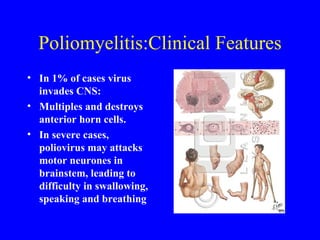
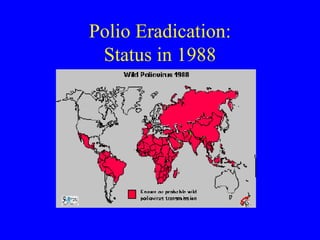
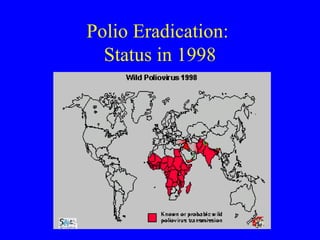
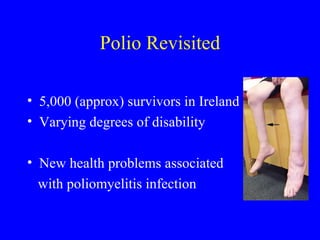
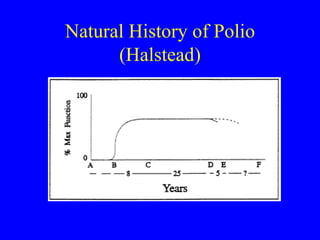
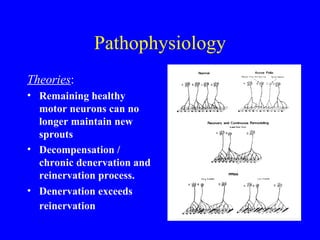
Poliomyelitis, or polio, is a viral disease that was a major cause of disability until widespread vaccination in the 1960s. Some polio survivors later develop Post-Polio Syndrome, characterized by new muscle weakness and fatigue decades after the initial infection. Management of Post-Polio Syndrome is multidisciplinary and focuses on symptom management through rehabilitation, orthotics, energy conservation, and treatment of comorbidities like sleep apnea. While polio has been eradicated in most countries, Post-Polio Syndrome remains an issue for aging polio survivors and further research is still needed.


































































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)











