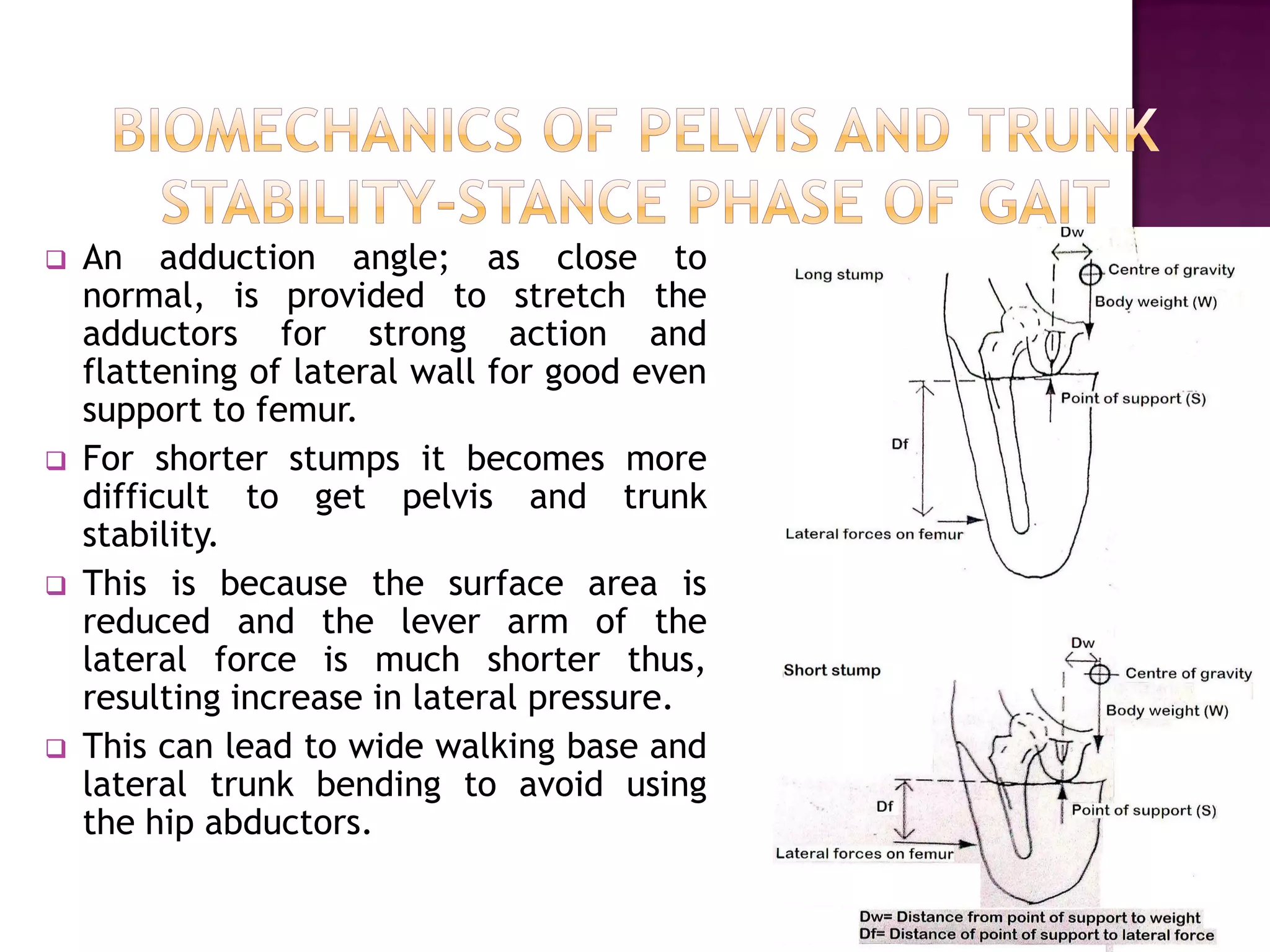
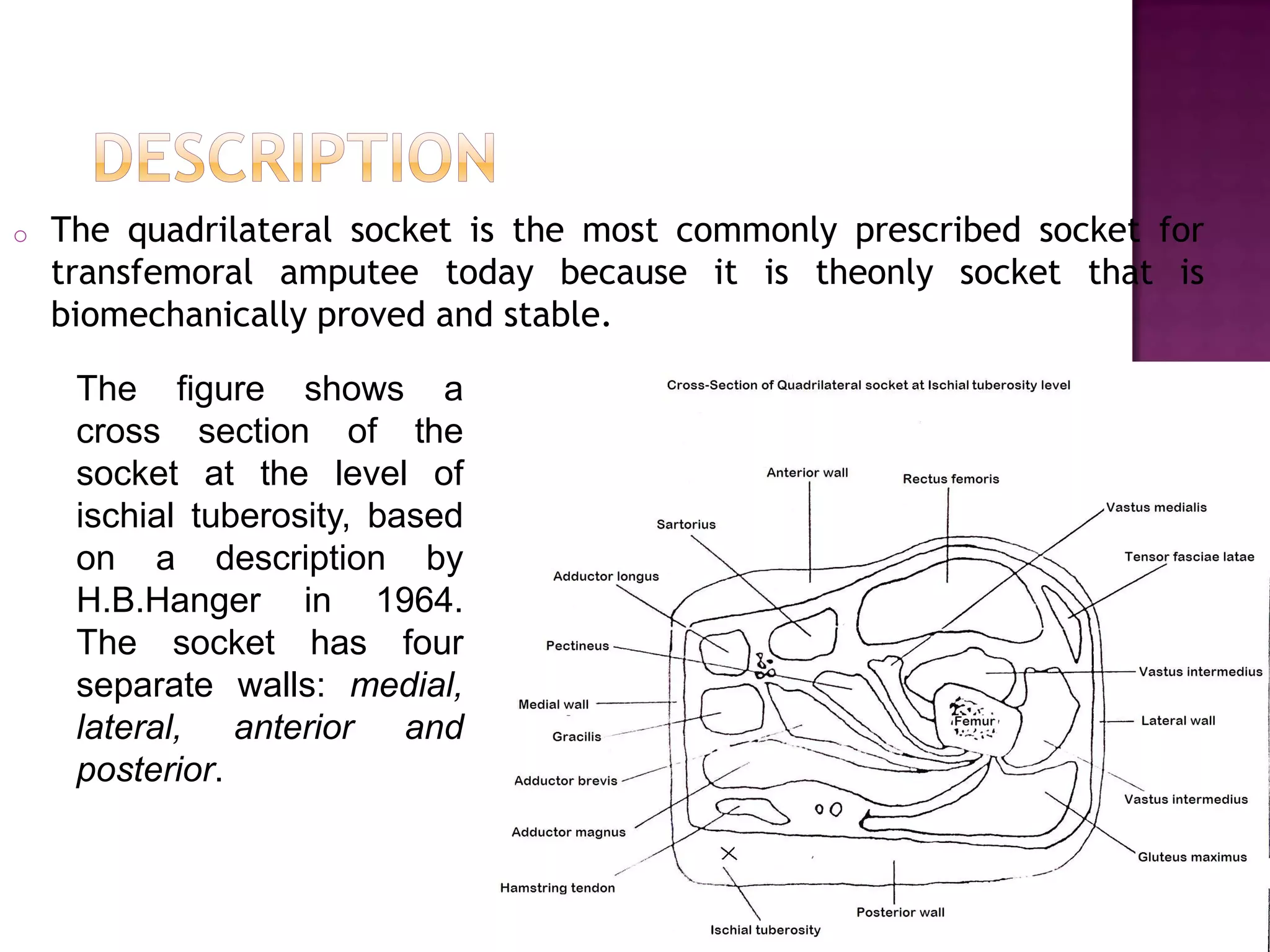
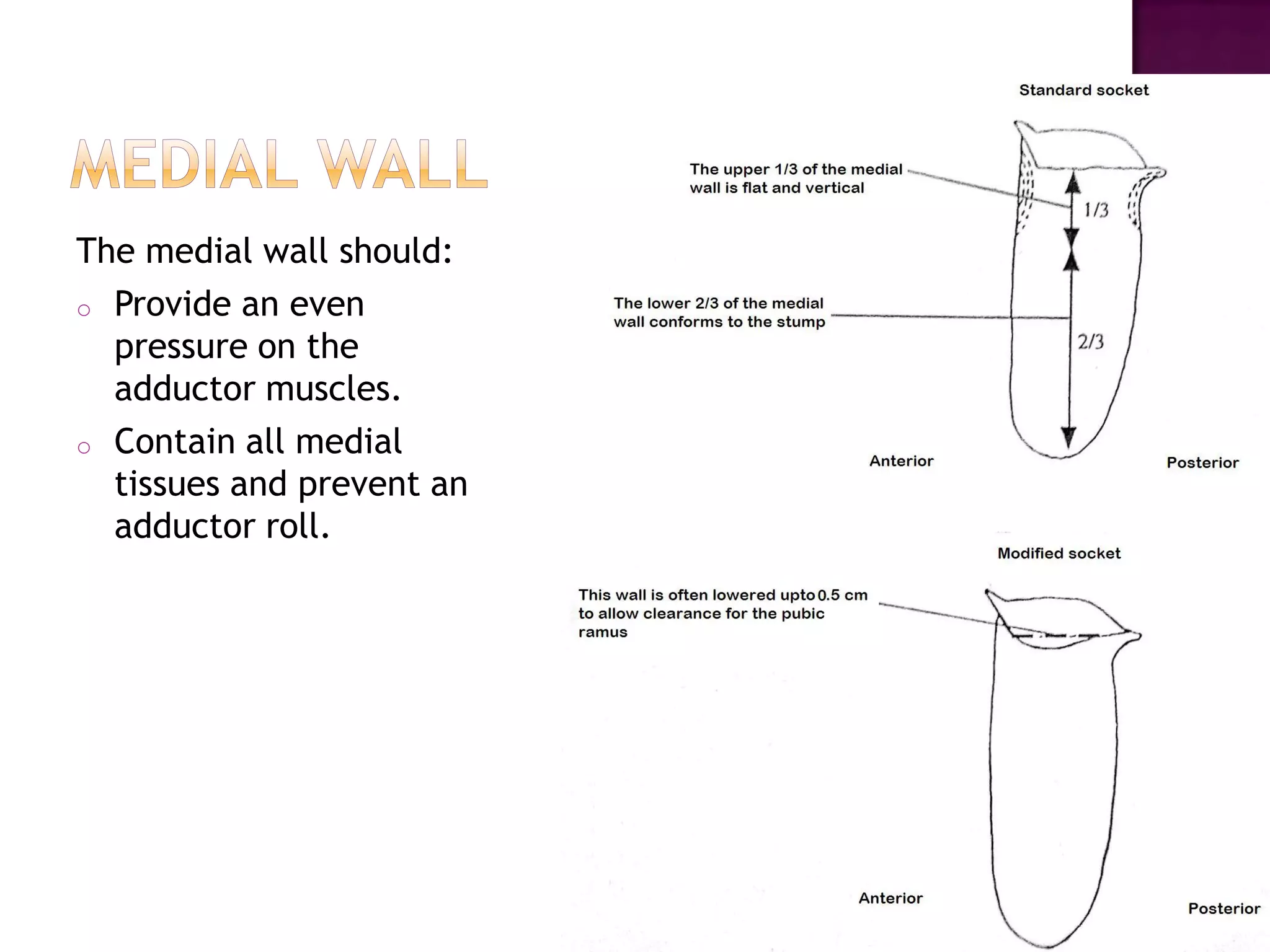
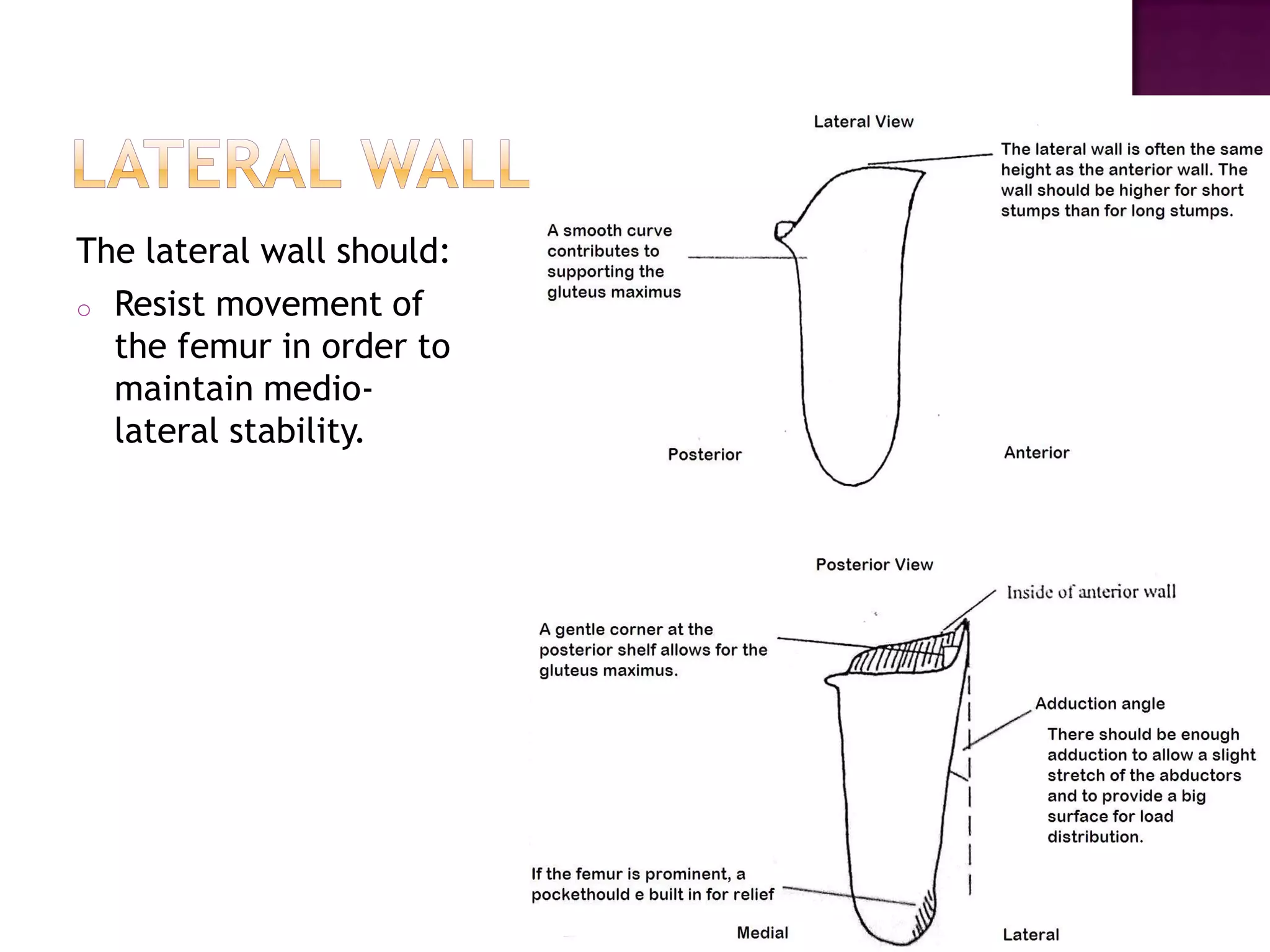
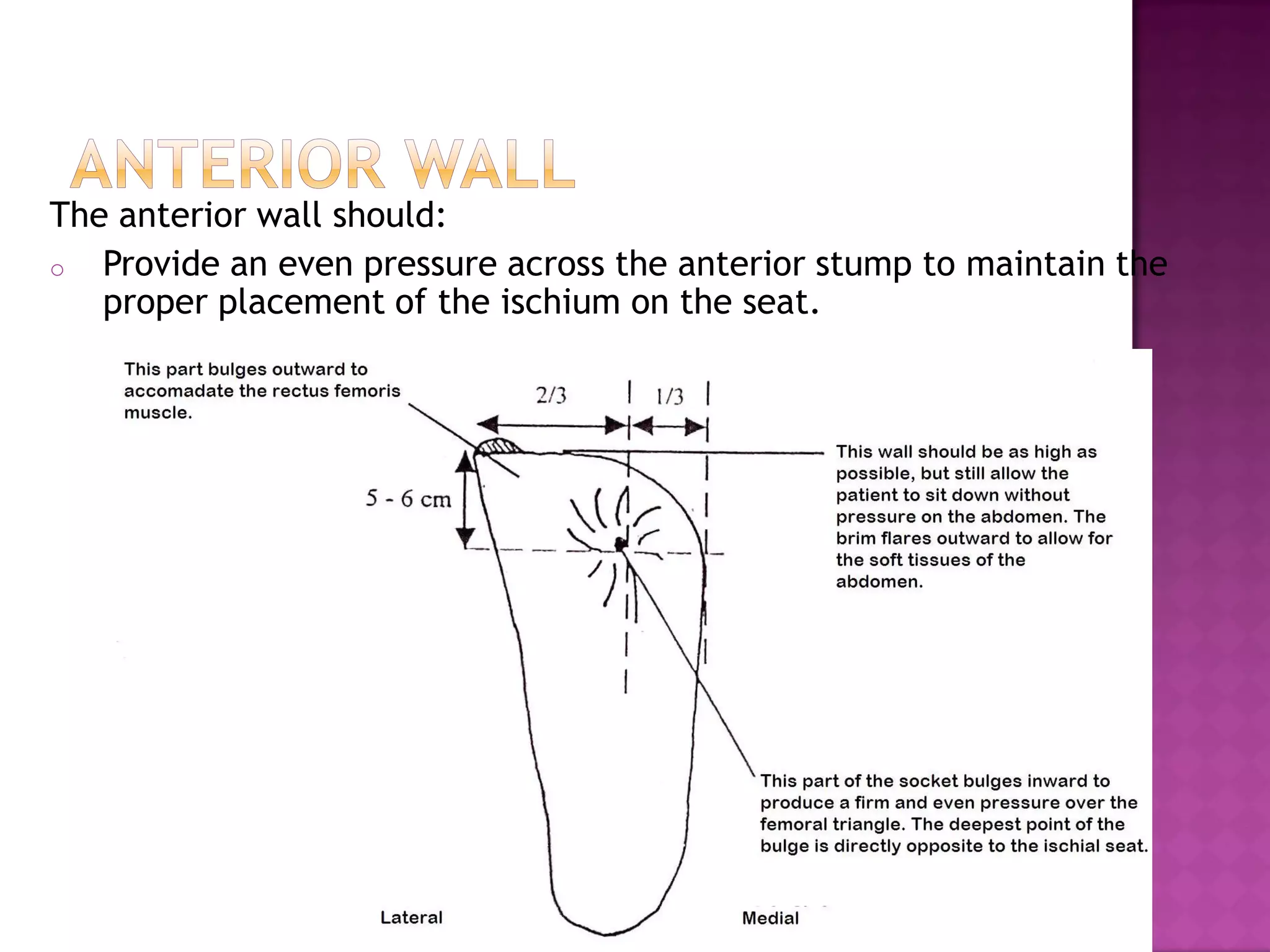
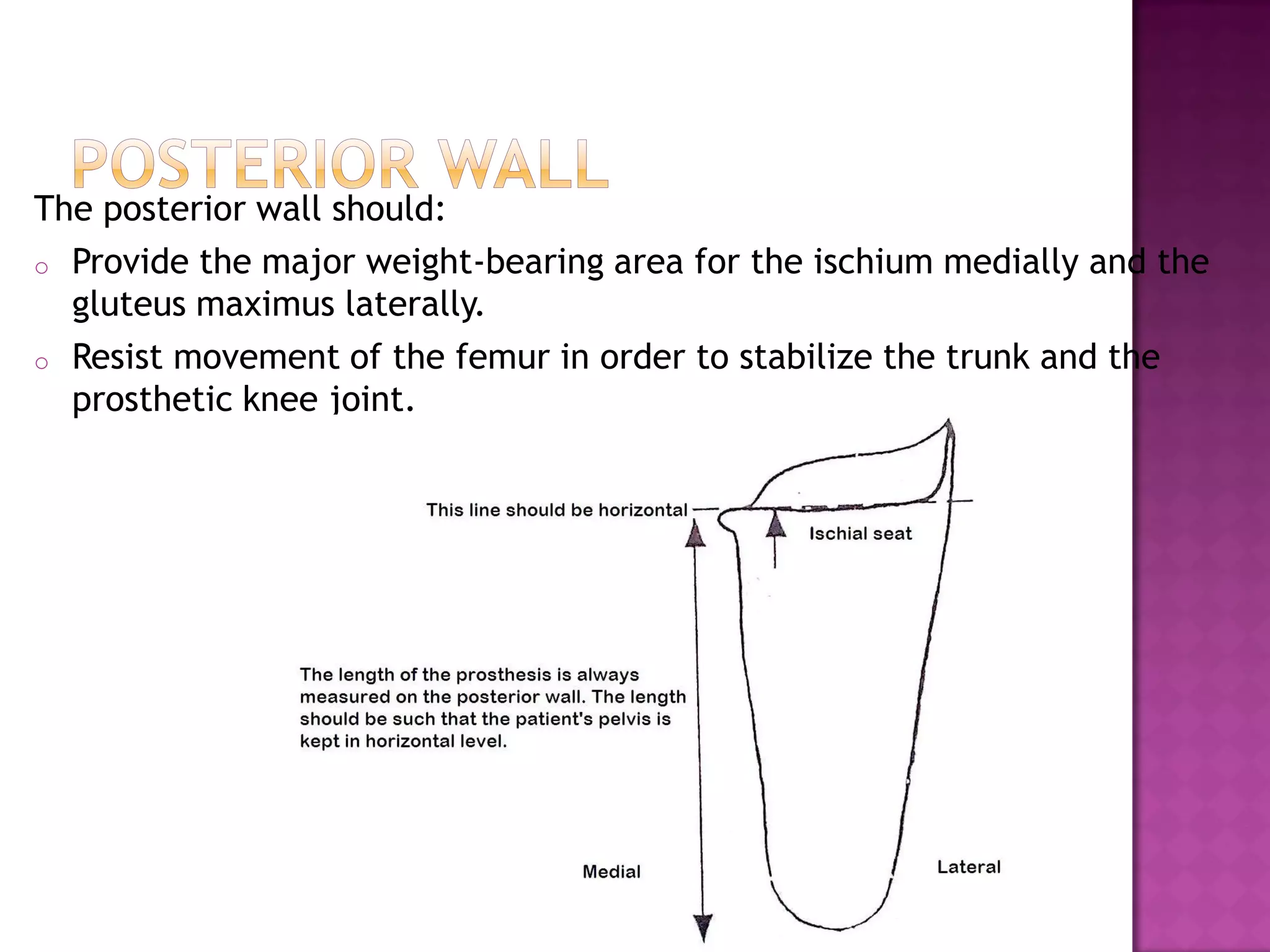
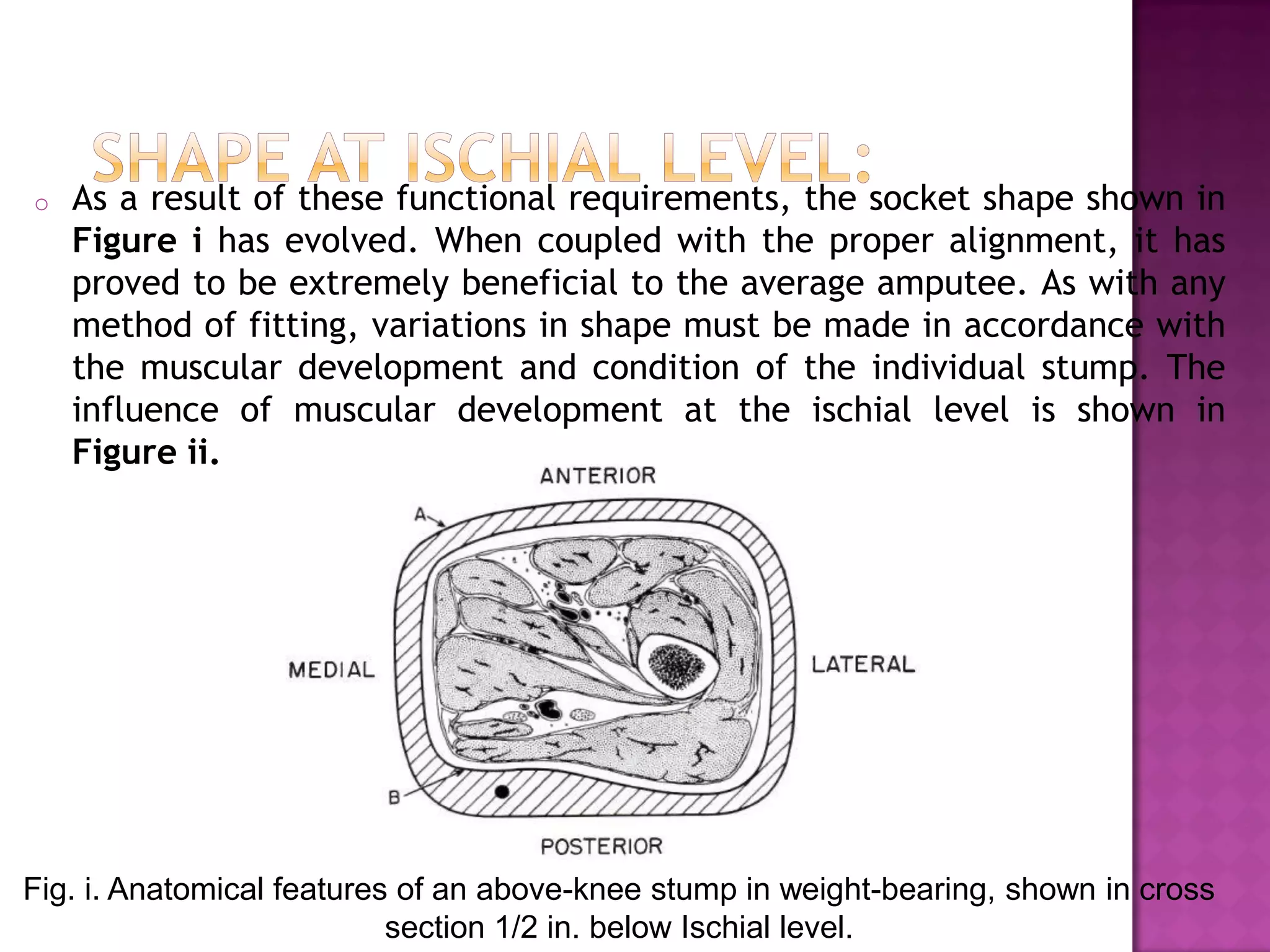
The document discusses the quadrilateral socket for transfemoral amputees. It describes the socket as having four walls - medial, lateral, anterior, and posterior - which provide stability and function. Each wall is contoured to stabilize specific muscles and bones. The quadrilateral socket allows for a narrow base of gait and medio-lateral stability when coupled with proper alignment. It remains the most commonly used socket design despite new techniques because it is biomechanically proven to be stable.