Downloaded 1,760 times


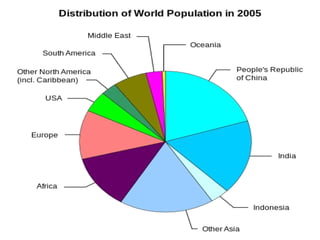

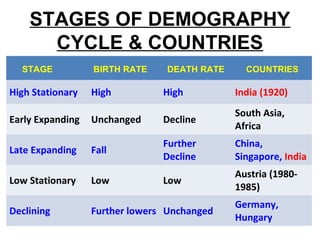
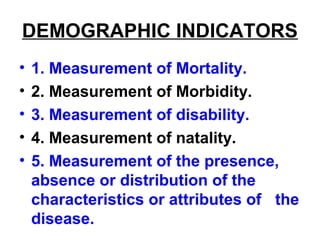
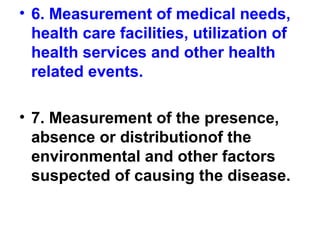
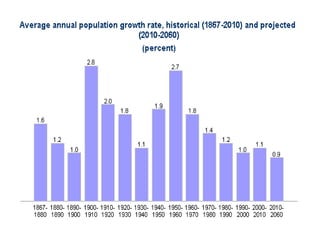


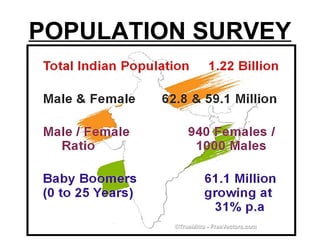




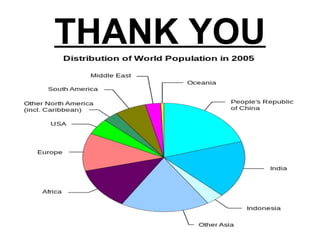

Demography is the statistical study of human populations. It examines the size, structure, and distribution of populations, as well as changes to them over time due to births, deaths, and migration. Key demographic indicators include birth rates, death rates, fertility rates, and life expectancy. Demographic data helps analyze population growth and structure.