Downloaded 942 times
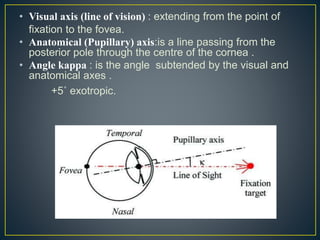
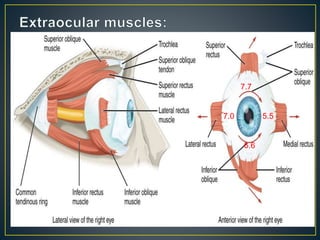
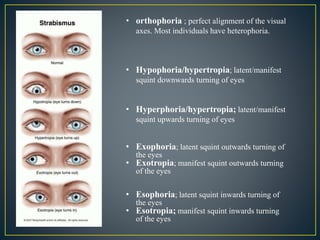
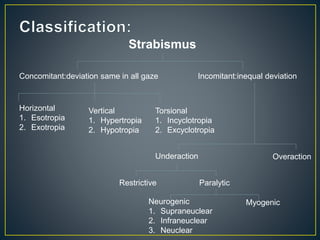
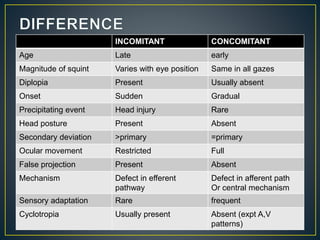

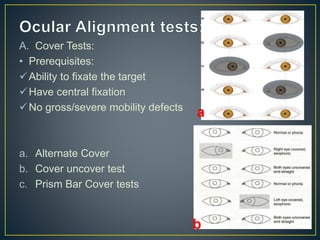
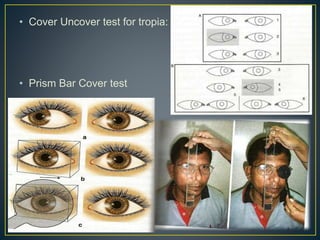
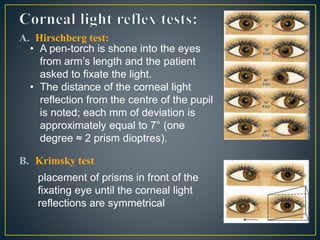
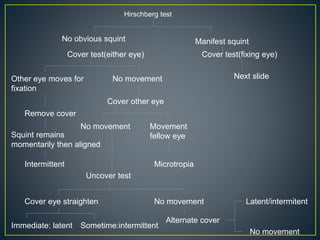
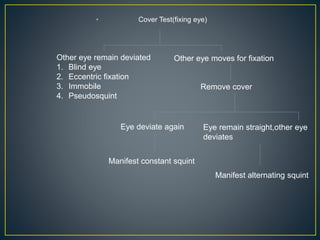
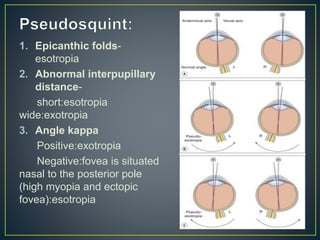
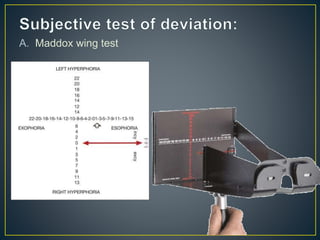
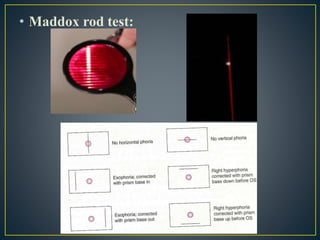
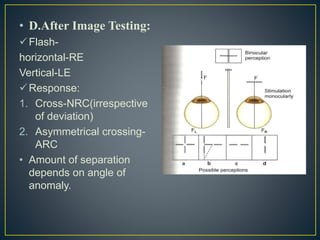
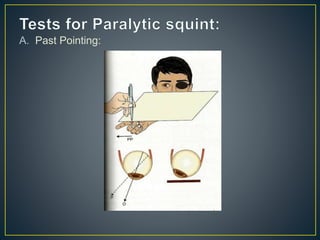
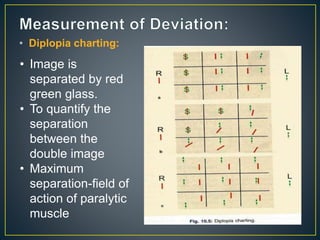
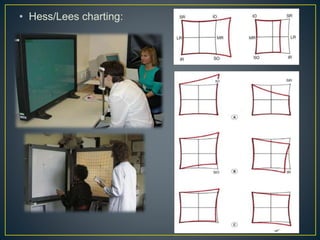


This document discusses strabismus, which is a misalignment of the visual axes of the eyes. It defines key terms like phoria, tropia, intermittent tropia, and provides details on the anatomical and visual axes. It describes various types of strabismus like concomitant, incomitant, horizontal, vertical, and torsional deviations. It also discusses the mechanisms, causes, adaptations, and evaluations of strabismus, including cover tests, versions, ductions, fusional amplitudes, stereopsis tests, and diplopia evaluation methods.












![Types of pediatric contact lens [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/typesofpediatriccontactlensautosaved-200210123904-thumbnail.jpg?width=640&height=640&fit=bounds)















































![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)













![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)


