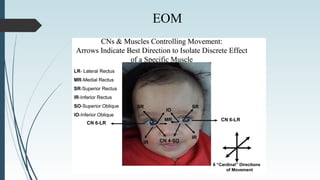
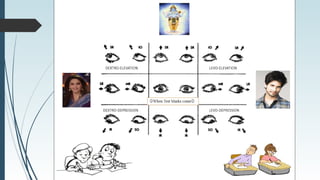
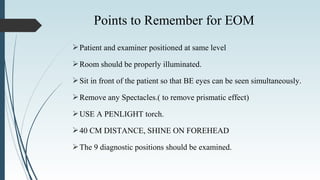
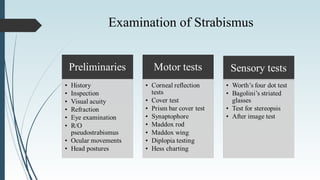
The document presents a comprehensive diagnostic evaluation for strabismus, outlining various axes of the eye, relevant anatomy, examination methods, and testing procedures. It details the importance of thorough patient history and examination techniques, including both subjective and objective tests for assessing ocular alignment and motility. Additionally, it highlights common misdiagnoses like pseudostrabismus and aims to provide a systematic approach to understanding and diagnosing strabismus effectively.