Downloaded 18 times

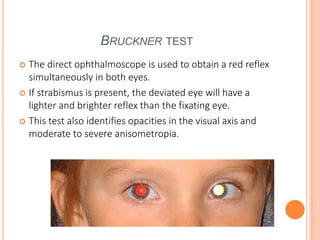
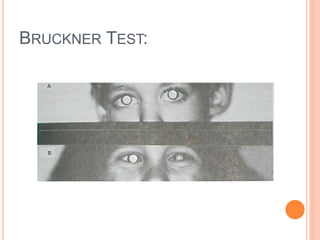
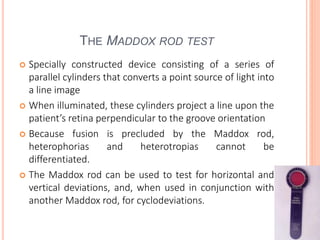

The document is a detailed assessment of ocular alignment and evaluation of eye movements, covering definitions, positions of gaze, and clinical methods for diagnosis. It discusses both subjective and objective testing methods, including cover tests, light reflex tests, and dissimilar image tests, for identifying strabismus and measuring deviations. Techniques like the Maddox rod test and the Bruckner test are highlighted for their role in diagnosing and quantifying eye alignment issues, aiming to assist clinicians in effective examination and treatment.























































































