Downloaded 257 times

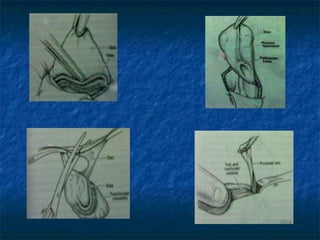


This document discusses congenital inguinal hernia and hydrocele. It notes that a congenital inguinal hernia occurs when the processus vaginalis fails to close after testicular descent in fetal development, allowing abdominal contents to enter the scrotum. It has a high rate in premature infants and is more common in males. A hydrocele occurs when the processus vaginalis remains fluid-filled but no abdominal contents enter. Both often resolve spontaneously in infants but may require surgery if persisting past 2 years. The hernia repair procedure involves high ligation of the hernia sac at the internal ring through an inguinal incision.











































































































