Downloaded 51 times

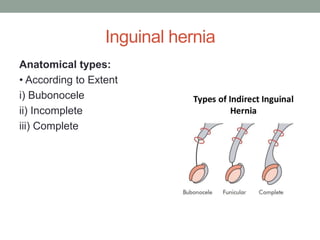
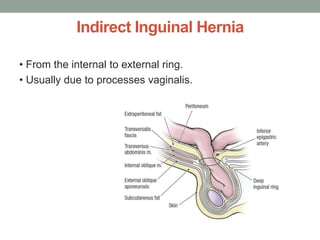
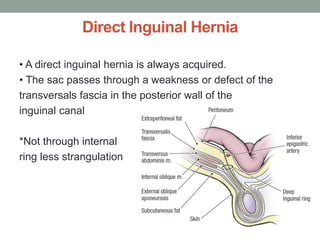
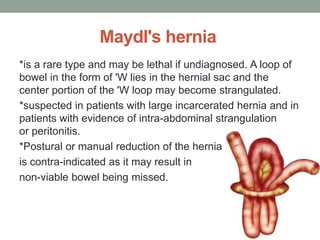
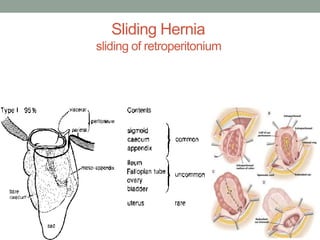
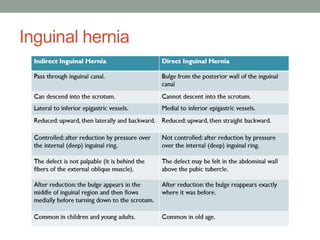
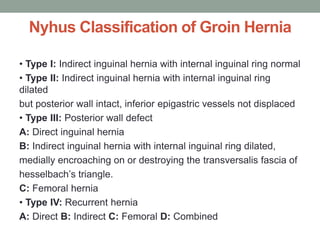
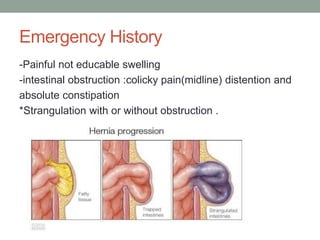
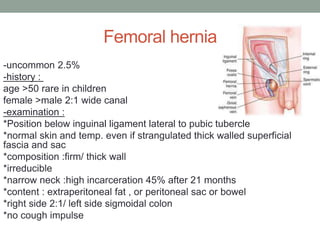
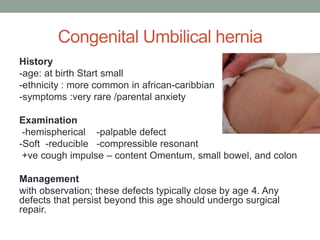

The document provides a comprehensive overview of hernias, including their definitions, classifications, and anatomical considerations. It discusses the various types of hernias, such as inguinal, femoral, umbilical, and lumbar, along with their causes, symptoms, and diagnostic approaches. Treatment options range from conservative management to various surgical techniques, highlighting the importance of proper diagnosis and treatment to prevent complications.





























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





