Downloaded 75 times

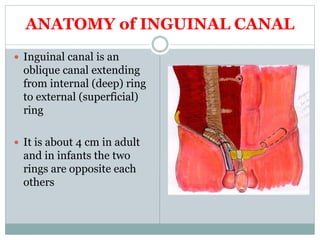
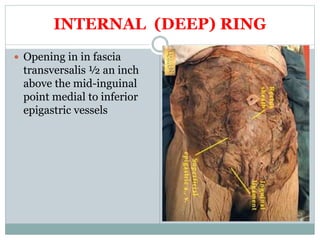
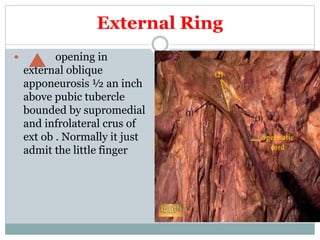
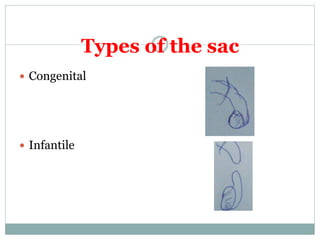
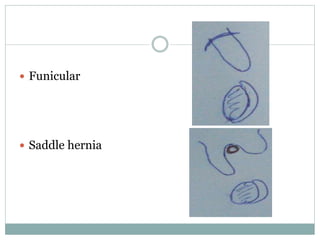
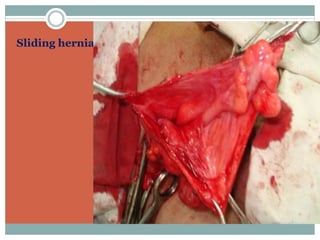
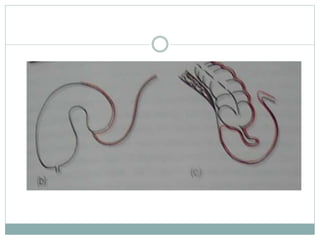
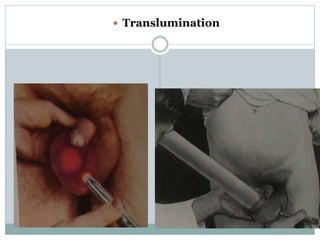
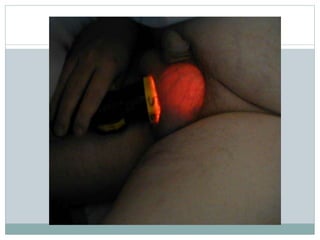
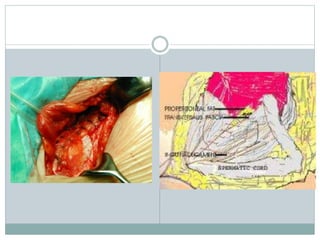
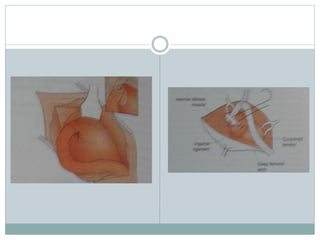
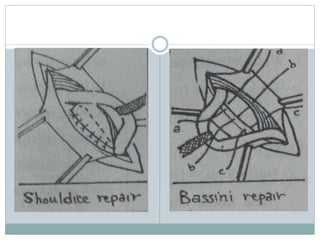
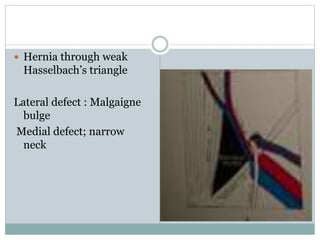
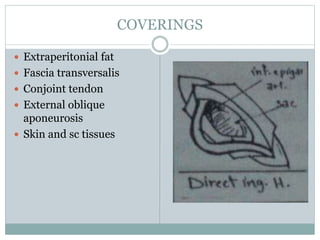










This document provides an overview of hernias and abdominal wall defects. It defines hernias as protrusions of an organ or tissue through a defect in the wall of the containing cavity. Various types of hernias are described including indirect inguinal, direct inguinal, femoral, umbilical, incisional and rare varieties. Factors that predispose to hernias as well as the anatomy, contents, coverings and complications of different hernias are discussed. Clinical features and treatment approaches are also summarized.






























































































