Downloaded 857 times
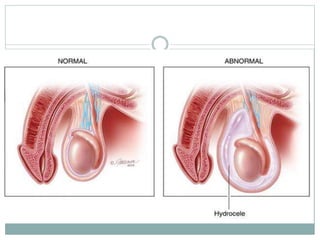

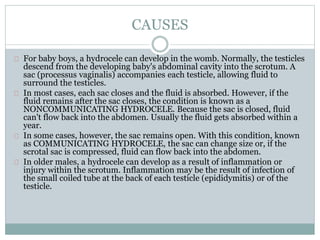
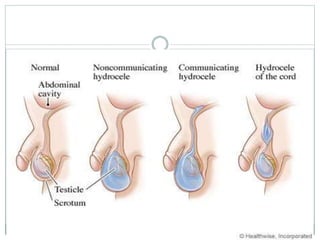

This document discusses hydroceles, which is an abnormal fluid collection in the scrotum. Hydroceles in infants are usually caused by incomplete closure of the processus vaginalis during development. For older boys and men, hydroceles can be idiopathic or caused by inflammation or injury in the scrotum. The document describes the causes, risk factors, signs and symptoms, diagnosis, and treatment of hydroceles. Treatment typically involves draining the fluid through a minor operation, with complications being rare.



























































































