Downloaded 622 times
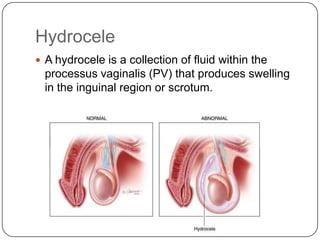

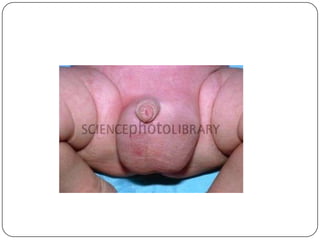


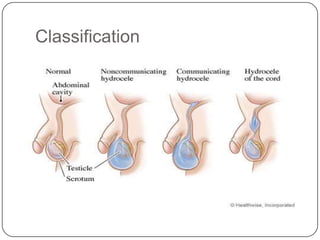
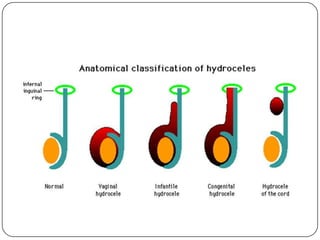
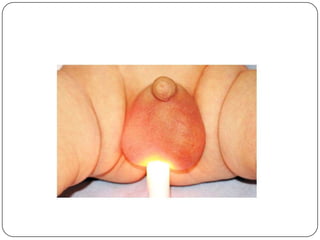



Hydrocele is a collection of fluid within the processus vaginalis that causes swelling in the scrotum. It is usually caused by a failure of the processus vaginalis to completely fuse during development. Hydroceles can be communicating or non-communicating depending on whether the processus vaginalis remains open to the abdominal cavity. The standard treatment is surgical repair to prevent the fluid from reaccumulating. Surgery involves ligating and removing the hydrocele sac to restore normal drainage from the scrotum. Complications are rare if the surgery is performed properly.




























































































