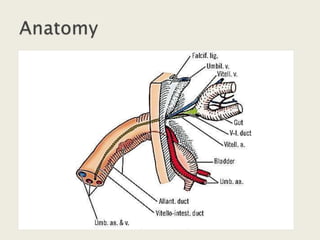
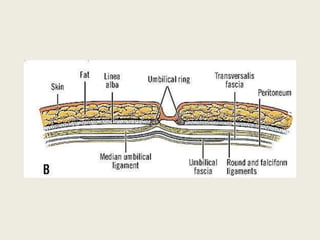
The umbilicus, or navel, is located along the linea alba and is the site of attachment for the fetal umbilical cord. The umbilicus can be affected by various congenital anomalies, inflammatory conditions, hernias, and neoplasms. Common disorders of the umbilicus include patent urachus, umbilical granulomas, hernias in infants and adults, and rare cases of primary or metastatic tumors. Evaluation and management depends on the specific condition but may involve antibiotics, surgery, or observation.