Downloaded 30 times

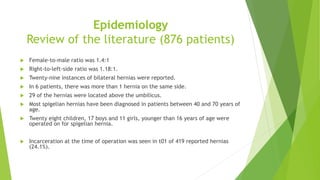




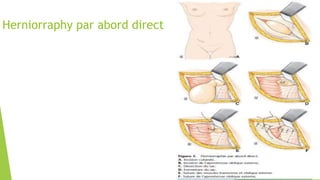


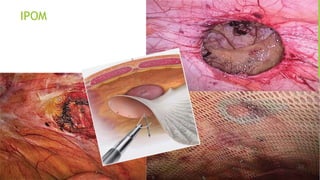
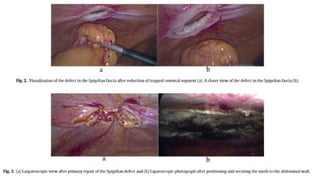




Spigelian hernia is a rare type of hernia that occurs in the Spigelian fascia of the abdominal wall. It was first described in the 17th century by Adriaan van den Spiegel. Spigelian hernias account for about 1% of all ventral hernias. They most commonly occur in adults ages 40-70 and present with pain. Diagnosis can be challenging as physical exam may not reveal a bulge. Imaging like ultrasound or CT can help identify the hernia defect. Treatment options include open herniorrhaphy or laparoscopic repair with mesh. Laparoscopy is preferred to minimize morbidity and allow for treatment of other hernias if present. Recurrence after












































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)






