Downloaded 1,278 times




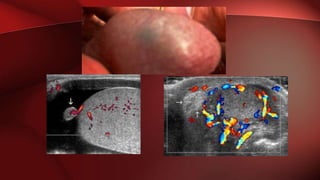

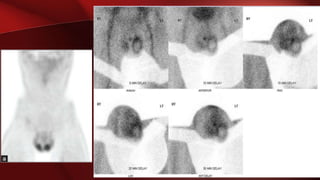
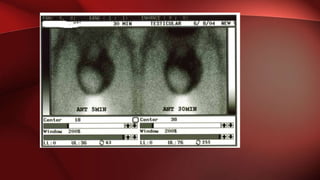

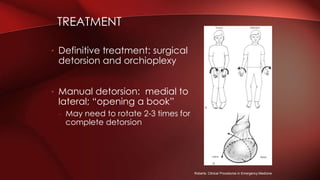


Testicular torsion refers to twisting of the spermatic cord and loss of blood supply to the testicle. It is a urological emergency as early diagnosis and treatment are needed to save the testicle. Ultrasound with Doppler is the primary imaging method and shows absent or decreased blood flow in the affected testicle compared to the normal side. Prompt surgical detorsion and orchioplexy are the definitive treatments.

















































































