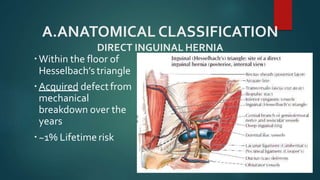
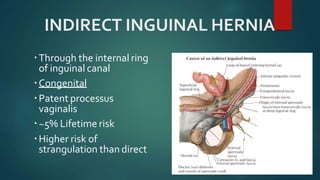
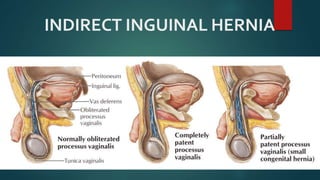
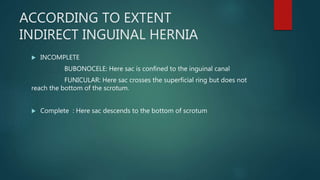
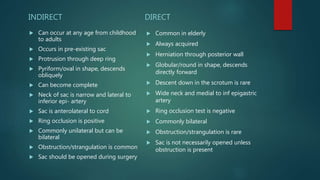
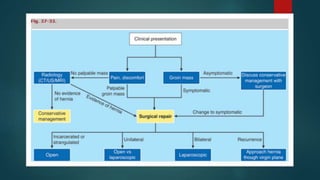
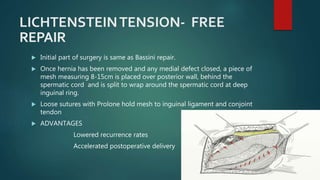
An inguinal hernia occurs when abdominal contents bulge through the inguinal canal. There are two main types - indirect which are congenital and direct which are acquired. Diagnosis is made through history and physical exam assessing for reducibility and impulse on coughing. Treatment options include watchful waiting for small reducible hernias or surgical repair through open or laparoscopic techniques. The Lichtenstein tension-free repair using mesh placement is commonly performed.






























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















