
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Case discussion uterine perforation
Similar to Case discussion uterine perforation (20)
More from Kavinda Hewawitharana
More from Kavinda Hewawitharana (20)
Recently uploaded
Recently uploaded (20)
Case discussion uterine perforation
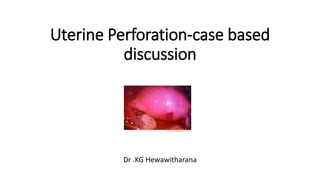
- 1. Uterine Perforation-case based discussion Dr .KG Hewawitharana
- 2. Case • Mrs .MH • 48 years • G3P3C3-all VDs & family completed + BL LRT • Ix for peri-menopausal bleeding characterized by frequent, irregular cycles associated with heavy menstrual loss for about 6/12 • On examination, pt had normal size uterus + cervix was healthy • TVS-ET=20mm • Planned for hysteroscopy + D&C
- 3. Surgery • Under GA • Lithotomy position & bladder emptied • Uterine sound passed- anteverted, normal size ut • Cervix dilated up to Hagar 8 • Hysteroscopy done- finding-fundal polyp • Polyp removed & curettage done • During this procedure-yellowish fatty tissues encountered and procedure stopped.
- 4. Action • Call for help-SR • Patient assessed • Decided to keep on IV AB, nil by mouth, IV fluids & planned for diagnostic laparoscopy following day. • Laparoscopy was done-no viscus injury other than perforated uterus in fundal region and omental tissues entering to perforation. • Since no active bleeding point, no further intervention was done.
- 5. Discussion-2013 TOG article based • Uterine perforation is uncommon, but potentially serious complication • Most common reason/cause is TOP • Uterine manipulation,ERPC,IUD insertion & Hysteroscopy are also known causes • Uteri that are likely for perforation in such procedure are postpartum or pregnant uteri, atrophic uteri, anomalous uteri, Infected uteri & retroverted uteri.
- 6. Incidence & sequalae • Out patient hysteroscopy-0.002-1.7% • Operative hysterocopy-1.6% • 15% of IUD insertion related perforation associate with viscus damage • 3-7.5% bowel injury noted in such instances • Most are at uterine body & small with little bleeding • If lower uterus or internal OS region got perforate major bleeding may occur • If instruments pass through damaged area, viscus or vascular damage is high
- 7. When to suspect • If instrument extend beyond the uterus with loss of resistance • Sudden loss of vision during hysteroscopy due to collapse uterus • Unusual bleeding with large deficit in distention medium • Direct visualization of perforation site • Visualization of bowel/omentum
- 9. Risk factors • 1.High risk uterus & cervix • 2.high risk surgery • 3.High risk surgeon
- 11. cont • 2nd trimester surgical TOP are 2 times more likely of having perforation than that of 1st trimester • Thus accurate POG estimation is important to plan sx • Also equally implicate with regard to ERPC following incomplete MC
- 12. High risk surgery ERPC for retained tissues in PPH (5%-6% cases) When intra uterine adhesions exist (0.07-1.8%) TOP (0.5%) PMB investigation with hysteroscopy (0.2-2%)
- 13. High risk surgeon • Very hard to find a gynecologist who had no experience with uterine perforation • Adequately trained surgeons less likely to cause perforations
- 14. Prevention • Risk assessment & adequate preparation • Risk management as explained valid consent, alert theater staff , keep ready laparoscope to use when necessary , get the involvement of experienced surgeons • Prior cervical preparation with misoprostol in premenopausal patients to reduce resistance.(no benefit in post menopausal) • Depend on individual scenarios, oral or vaginal PG use prior to surgical TOP reduce dilation force, trauma & bleeding • Adequate, gradual cervical dilation with half sized dilators avoiding excessive force
- 15. cont • Hawkins-amber Vs Hagar- former is safe and better as it needs less force
- 16. cont • USS guided procedure • Under vision of Laparoscopy when concomitant abdominal procedure happens
- 17. Management
- 18. cont • Mx depend on type of procedure & instruments used for it • If perforation is due to a dilator,curette,polyp forcep,IUD or 5mm hysteroscope- antibiotics & observation alone sufficient • If larger instruments used & bleeding noted-laparoscopy is needed • If during TOP/ERPC-again laparoscopy is necessary and get the involvement of surgeons as there may be bowel injury • It is important to place a catheter for fluid balance monitoring & to identify possible bladder injury if hematuria noted
- 19. Furthermore • If it is a small perforation, often no intervention is required and may use diathermy for bleeding arrest in laparoscopy • Meanwhile if the original procedure is incomplete, under direct vision this has to be perform, thus further injury can be avoided • Consider laparotomy if continuing bleeding, enlarging broad ligament hematoma, when it needs to close uterine peroration but difficult with laparoscopy • But try as much as possible for laparoscopic closure • Hysterectomy is likely if identification & intervention gets delayed because patient deteriorate with bleeding while edematous tissues make interventions more difficult.
- 20. POST OP • IV AB for 24 hrs & keep admit for 24hrs • If stable can send home • R/V if ny symptom • Because-though early observation shows stable vital signs + normal bowel sounds, subsequent symptoms of bowel injury will manifest much later • Document & debrief