This document discusses the management of non-tubal ectopic pregnancies. It begins by defining ectopic pregnancies and providing brief history. It then discusses the various types of non-tubal ectopic pregnancies including interstitial, abdominal, ovarian, cervical, heterotopic, and cesarean scar ectopic pregnancies. For each type, it covers etiology, presentation, diagnosis, and treatment options. Conservative and surgical management approaches are described. The document provides a comprehensive overview of rare forms of ectopic pregnancy.
under and post graduate best presentation ever about the assisted vaginal delivery,operative vaginal delivery, or instrumental vaginal delivery.
done by waill salan al.timeemi/stager 2014-2015/ Iraq-al.qadisiyyah college of medicine.
Preterm labor is the labor that starts before the 37th completed week. In this presentation, we will discover causes, pathogenesis, diagnosis, clinical features, and management principles for preterm labor along with the most recent evidence.
under and post graduate best presentation ever about the assisted vaginal delivery,operative vaginal delivery, or instrumental vaginal delivery.
done by waill salan al.timeemi/stager 2014-2015/ Iraq-al.qadisiyyah college of medicine.
Preterm labor is the labor that starts before the 37th completed week. In this presentation, we will discover causes, pathogenesis, diagnosis, clinical features, and management principles for preterm labor along with the most recent evidence.
accurate assessment of gestational age by certain mensrtual data and clinical examination may have dating discrepancy with the ultrasound. this ppt critically addresses such issues
A case report of cervical ectopic pregnancy misdiagnosed as cervical miscarriageApollo Hospitals
Cervical pregnancy is a rare variety of ectopic gestation. The aetiology is obscure. Diagnosis may be difficult unless the clinician/the radiologist is conscious of the entity. The evaluation of first trimester vaginal bleeding or pelvic pain is an important task for the emergency physician. The early identification of an ectopic pregnancy can help prevent significant morbidity and mortality for patients seeking emergency care. We present the case of a patient found to have a cervical ectopic pregnancy.
accurate assessment of gestational age by certain mensrtual data and clinical examination may have dating discrepancy with the ultrasound. this ppt critically addresses such issues
A case report of cervical ectopic pregnancy misdiagnosed as cervical miscarriageApollo Hospitals
Cervical pregnancy is a rare variety of ectopic gestation. The aetiology is obscure. Diagnosis may be difficult unless the clinician/the radiologist is conscious of the entity. The evaluation of first trimester vaginal bleeding or pelvic pain is an important task for the emergency physician. The early identification of an ectopic pregnancy can help prevent significant morbidity and mortality for patients seeking emergency care. We present the case of a patient found to have a cervical ectopic pregnancy.
In this presentation we will discuss
First trimester US especially TVS is an integral part for confirmation of intrauterine pregnancy and to rule out ectopic pregnancy.
First trimester US helps us in suggesting conceptus viability.
First trimester US especially TVS is very efficient in approaching and evaluating the cause of vaginal bleeding.
This describes the ultrasound findings in various types of ectopic pregnancies. This also goes on to integrate Beta hCG into the diagnostic algorithm of ectopic pregnancy. The lecture also briefly introduces the use of progesterone levels in the diagnostic work-up of ectopic pregnancy.
In ectopic pregnancy, implantation occupies at a site other than the endometrium. Ectopic pregnancies are responsible for approximately 10 percent of all maternal mortality. The prognosis for future reproduction is poor. Only one half of women having an ectopic pregnancy are eventually delivered of a liveborn infant. Various factors contribute to ectopic pregnancies, the most common being infection. Unlike intrauterine spontaneous abortions, genetic factors are not paramount in the etiology of ectopic pregnancy.
Cervical incompetence is the inability for the cervix to retain an intra-uterine pregnancy till term as a result of structural and functional defects of the cervix
Obstetrical Ultrasound• Introduced in the late 1950’s ultrasonography is a safe, non- invasive, accurate and cost-effective means to investigate the fetus• Computer generated system that uses sound waves integrated through real time scanners placed in contact with a gel medium to the maternal abdomen• The information from different reflections are reconstructed to provide a continuous picture of the moving fetus on the monitor screen
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
Lung Cancer: Artificial Intelligence, Synergetics, Complex System Analysis, S...Oleg Kshivets
RESULTS: Overall life span (LS) was 2252.1±1742.5 days and cumulative 5-year survival (5YS) reached 73.2%, 10 years – 64.8%, 20 years – 42.5%. 513 LCP lived more than 5 years (LS=3124.6±1525.6 days), 148 LCP – more than 10 years (LS=5054.4±1504.1 days).199 LCP died because of LC (LS=562.7±374.5 days). 5YS of LCP after bi/lobectomies was significantly superior in comparison with LCP after pneumonectomies (78.1% vs.63.7%, P=0.00001 by log-rank test). AT significantly improved 5YS (66.3% vs. 34.8%) (P=0.00000 by log-rank test) only for LCP with N1-2. Cox modeling displayed that 5YS of LCP significantly depended on: phase transition (PT) early-invasive LC in terms of synergetics, PT N0—N12, cell ratio factors (ratio between cancer cells- CC and blood cells subpopulations), G1-3, histology, glucose, AT, blood cell circuit, prothrombin index, heparin tolerance, recalcification time (P=0.000-0.038). Neural networks, genetic algorithm selection and bootstrap simulation revealed relationships between 5YS and PT early-invasive LC (rank=1), PT N0—N12 (rank=2), thrombocytes/CC (3), erythrocytes/CC (4), eosinophils/CC (5), healthy cells/CC (6), lymphocytes/CC (7), segmented neutrophils/CC (8), stick neutrophils/CC (9), monocytes/CC (10); leucocytes/CC (11). Correct prediction of 5YS was 100% by neural networks computing (area under ROC curve=1.0; error=0.0).
CONCLUSIONS: 5YS of LCP after radical procedures significantly depended on: 1) PT early-invasive cancer; 2) PT N0--N12; 3) cell ratio factors; 4) blood cell circuit; 5) biochemical factors; 6) hemostasis system; 7) AT; 8) LC characteristics; 9) LC cell dynamics; 10) surgery type: lobectomy/pneumonectomy; 11) anthropometric data. Optimal diagnosis and treatment strategies for LC are: 1) screening and early detection of LC; 2) availability of experienced thoracic surgeons because of complexity of radical procedures; 3) aggressive en block surgery and adequate lymph node dissection for completeness; 4) precise prediction; 5) adjuvant chemoimmunoradiotherapy for LCP with unfavorable prognosis.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
2. Contents
1. Introduction
2. Interstitial Pregnancy
3. Abdominal Pregnancy
4. Ovarian EP
5. Cervical EP
6. Heterotopic pregnancy
7. cesarean scar ectopic pregnancy (CSP)
8. PUL
9. References
3. Introduction
• Derived from the Greek word ektopos, meaning out of
place
• Ectopic pregnancies were initially described in the
10th century (Albucasis in 936-1013 A.D.)
• In 1693 Boucier noted the presence of ectopic
pregnancy at postmortem examination of an executed
prisoner
• A more complete report was made in 1731
• for a long time were universally fatal events for the
mother
4. ….cnt’d
• Nontubal ectopic pregnancies accounts for only 5 % of
all EPS, yet they account for 20 % of the fatalities
• Traditionally diagnosed late and have been associated
with significant morbidity and mortality
• Over recent years increase in the early diagnosis of
non-tubal ectopic pregnancies
• Management has now progressed from open surgical
management to the use of minimal access techniques
and the exploration of medical and conservative
treatments either alone or as adjuvant therapies
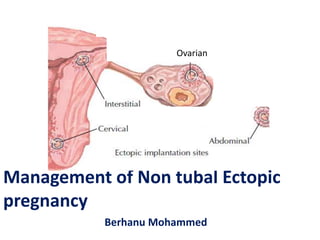
5. Sites of implantation of 1800 ectopic pregnancies from a 10-year population-
based study. (Data from Callen, 2000; Bouyer and colleagues, 2003.)
8. Diagnosis
• Short period of Ammenorrhea , pain and vaginal
bleeding(slight, brownish, continouse , clots rarely)
• Pain in epigastrium and shoulder(acute bleeding)
• History of PID, Use of IUD
• History of sterility
• Palpable mass , tenderness in the pelvis, enlarged
ux
• Cervical motion tenderness
9. …cnt’d
Signs
• Adler’s sign-fixed abdominal
tenderness
• Bath room sign-pain on
defaecation or perineal discomfort
manifest as inability to sit square
on hard seat
• Cullen’s sign-periumblical
ecchymosis from intraperitoneal
bleeding
• Davis’s sign- subdiaphragmatic
space – shoulder tip pain
• Murphy’s sign- blood along the
urachus to umbilicus bruise
10. …cnt’d
Lab findings
• Hgb /Hct is falling
• HCG test -75% positive
• Leucocytes <20,000, mostly only slight
increased but ESR rises
Currettage
X-ray
11. …cnt’d
ULTRASONOGRAPHY
• At defined hCG titers, ultrasonography is excellent
for identifying an IUP.
• Transabdominal ultrasound : detects GS by 5 – 6 wks
Detects fetal heart activity at 7 wks of gestation.
Detects IUP at β-hCG of 6000 to 6500 mIU/ml
• Transvaginal ultrasound : detects IUP 1 wk earlier
than transabdominal U/S. It diagnosis IUP in the
range of 1500 to 2000 mIU/ml hCG.
12. …cnt’d
Culdocentesis
• Positive tap - aspiration of
at least 0.5ml non clotting
blood that has a Hct of
15%
– obtained in 70-90% of
patients with EP.
• Negative tap - aspiration
of at least 0.5ml of serous
fluid.
• Nondiagnostic - Failure to
aspirate any fluid -the
needle is not in the cul-de-
sac
13. …cnt’d
Laparascopy
• Is the gold standard for diagnosis
• Used when diagnosis is uncertain
• Direct visualization of pelvic organs offer a
reliable diagnosis.
• Compared with laparotomy, laparoscopy is
more cost - effective
14. Interstitial Pregnancy
• The proximal portion that lies within the muscular wall
of the uterus. It is 0.7 mm wide and approximately 1–2
cm long
• Rare condition,
• Accounts for no more than 2% to 4% of all tubal
pregnancies, a mortality rate in the range of 2.0–2.5%.
• Occurs once every 2,500 to 5,000 live births
• Gestational sac is better protected in the interstitial
than in other portions of the tube
• symptoms of interstitial ectopic pregnancies may
manifest later (>12 gestational weeks)----myometrial
distensibility
15. …cnt’d
• Pelvic pain and vaginal spotting are common
early symptoms
• Most of the same risk factors for interstitial
pregnancy are similar to those for ectopic
pregnancy in general
• PID, previous pelvic surgery and the use of
ART
• Ipsilateral salpingectomy is unique risk factor,
occurring in 37.5% of patients
16. Diagnosis
• critical evaluation of all the criteria used for
other types of tubal pregnancy
• includes acute abdominal pain, intraperitoneal
bleeding, a low hematocrit, and a positive
serum or urine pregnancy test
• sensitive β-hCG immunoassay and vaginal
ultrasonography
• Asymmetry of the uterus
17. Timor-Tritsch and colleagues established
TVU criteria
• An empty uterine cavity,
• A chorionic sac seen separately and >1 cm from the
most lateral edge of the uterine cavity, and
• A thick myometrial layer surrounding the chorionic
sac.
• "Interstitial line sign“ echogenic line extending from
endometrial cavity into the cornual region & abutting
the gestational sac
Specificity (88% to 93%), sensitivity (only about 40%)
for the diagnosis of interstitial pregnancy
18. Treatment
• Traditionally, the treatment of cornual
pregnancy has been hysterectomy or cornual
resection at laparotomy
• Depends on the extent of trauma that has
occurred in the uterine wall and on the
interest of the patient in preserving her
fertility
20. …cnt’d
Hysteroscopic procedures
• Hysteroscopic endometrial resection under
laparoscopic control
• Hysteroscopic cornual evacuation aided by polyp
forceps under ultrasound (USS) or laparoscopic
guidance
Medical
• Systemic methotrexate
• USS guided methotrexate
• Laparoscopic guided methotrexate/potassium chloride
• Systemic methotrexate followed by selective uterine
artery embolisation
21. Key points for medical treatment
• Haemodynamic stability is an essential
prerequisite for medical management.
• There should be no signs of rupture.
• The woman should be well motivated to
attend for regular (perhaps prolonged) follow-
up.
• There should be no medical contraindications
to methotrexate.
23. Abdominal pregnancies
• Very Rare,0.9- 1% all EP
• Ranging from 1 in 3,371 deliveries to greater than
1 in 10,200 deliveries
• Maternal mortality risk 7.7 times tubal EP, 90x
greater than IUP
– 5.1 per 1000 cases
• Classified as primary or secondary
• Most are secondary, the result of early tubal
abortion, rupture or ovarian abortion with
secondary implantation of the pregnancy into the
peritoneal cavity
24. Primary Abdominal pregnancy
• rare event, first true primary peritoneal pregnancy
described by Gallabin, 1903
Must meet the three criteria defined by Studdiford in 1942:
1. Both tubes and ovaries must be in normal condition with
no evidence of recent or remote injury.
2. No evidence of uteroperitoneal fistula should be found.
3. The pregnancy must be related exclusively to the
peritoneal surface and
4. early enough to eliminate the possibility that it is a
secondary implantation following a primary implantation
in the tube.
• ???? Helpful diagnosis or management.
25. Dx
Made usually intraoperatively (hx, P/E and Ix)
• Recurrent abdominal discomfort,
• Fetal movement beneath the abdominal wall, and
• Presence of fetal movements high in the upper
abdomen
• Cessation of fetal movement,
• Vomiting late in pregnancy,
• Fetal malposition,
• Closed and uneffaced cervix, or the
• Failure of oxytocin to stimulate the gestational mass
26. Dx …cnt’d
• Fetal small parts in the lateral position overlying the
maternal spine was first noted by Weinberg and
Sherwin in 1956
• A plain abdominal X-ray may reveal the fetus to be
separate from the uterus and the finding of bowel
shadows amid the fetus is said to be pathonomonic
• Ultrasound can usually identify an abdominal gestation
as separate from the nonpregnant uterus
• MRI, if U/S is unequivocal
• serum a-fetoprotein
27. characteristics of abdominal
pregnancy on ultrasound
• Presence of a fetus outside the uterus
• Absence of the uterine wall between the bladder and the
fetus
• Extrauterine location of the placenta
• poor visualization of the placenta
• pseudo-placenta previa appearance
• Oligohydramnios
• Fetal parts adjacent to the mother’s abdominal contents
• Abnormal fetal presentation, and
• The absence of amniotic fluid between the fetus and
placenta
29. …cnt’d
• MRI is becoming the investigation of choice in
suspected abdominal pregnancy
• Hysterosalpingography is reserved for cases
where fetal death has been confirmed
30. Complications
• Massive bleeding, Anemia
• Pelvic abscess
• Peritonitis
• Sepsis
• DIC
• Pulmonary embolism
• Massive rectal bleeding or
rectal passage of fetal bones
• MM 4% to 29%
• Fetal mortality is notoriously
high, ranging from 75% to 95%
of all cases
31. When to operate
• Immediate laparotomy before viability
• Between the 28th and 34th weeks controversial
with alive fetuse
• For dead fetus waiting for 8weeks if there is no
evidence of infection
• In cases with a live foetus near to obstetric
viability, to delay the operation in the hope of
obtaining a live baby
• The patient must be hospitalized as soon as the
diagnosis is suspected
32. Prerequisites for conservative
approach
• absence of fetal malformation;
• absence of maternal or fetal decompensation;
• continued surveillance of fetal well-being;
• placental implantation low in the abdomen, far
away from the liver or spleen;
• adequate amniotic fluid;
• continuous hospitalization in an appropriate
facility; and
• informed consent from the patient
33. Management
• Preoperative preparation include
• an adequate supply of compatible blood and blood
products
• appropriate intravenous infusion lines that can
deliver large amounts of fluid quickly
• surgical team should be standing by (bowel, vascular,
or genitourinary)
• Anti-shock trousers and autotransfusion apparatus
should also be available
• bowel preparation and prophylactic antibiotic
administration in preparation for surgery
34. Placenta management
• Still controversial
• Most clinicians believe the best treatment is
• to clamp the cord
• to leave the placenta in situ, and
• to close the abdomen, but to allow retroperitoneal drainage if
possible
• Can be removed after complete cessation of function is
demonstrated by quantitative β-hCG titers
• Removed during laparotomy only if it is accessible and if
its removal can be accomplished without excessive blood
loss
• MTX
35. Factors that favour primary removal
• Early gestation and therefore a smaller and less
vascular placenta;
• placental invasion that is confined to removable
organs such as tube, ovary and uterus;
• foetal death with probable thrombosis of most of the
placental vessels;
• attachment of the placenta to the broad ligament;
and
• severity of any haemorrhage present and the
effectiveness of haemostatic measures already
applied
36. Ovarian Ectopic Pregnancy
• 1 in 10 000 pregnancies; they account for 0·5–
3 per cent of all ectopic pregnancies
• may be primary or secondary and diagnosis is
seldom made prior to surgery
• associated with neither PID nor infertility
• DDX (1) haemorrhagic ovarian cyst, and (2)
ruptured corpus luteum cyst
37. …cnt’d
The etiology and pathogenesis of OP two seem to
be the most responsible causes:
• primary OP with intra-follicle fertilization
• retrograde flow in the fallopian tube of the
fertilized ovum released on to the ovary
Clinical picture
• same as that of a tubal ectopic, but
• degree of haemorrhage and haemoperitoneum
more sever
38. Diagnosis
Based on Spiegelberg’s criteria formulated in 1878.
The criterion states that:
(1) The tube on the affected side must be intact.
(2) The fetal sac must occupy the position of the
ovary.
(3) The ovary must be connected to the uterus by
the ovarian ligament.
(4) Definite ovarian tissue must be found in the sac
wall.
39. …cnt’d
• Most difficult
• does not always present by the triad of period of
amenorrhoea, per vaginal bleeding and pelvic
pain/tenderness/ cervical excitation
• persistent pelvic pain alone, a symptom not
always easily related to its cause, is the most
frequent clinical manifestation of an ovarian
gestation
• Haemothorax (4 case reports RT side
haemothorax )
• ovarian pregnancy does not recur
40. Management
Conservative Mx: Important because these patients are
usually young, healthy, fertile & desire future
childbearing.
Medical Management
Systemic methotrexate
• unruptured ovarian pregnancy
• no significant hemoperitoneum
• hemodynamically stable patient
Localized surgical resection
• ovarian wedge resection or
• cystectomy
41. …cnt’d
Laparoscopy : used to resect or perform laser
ablation of ovarian pregnancies
Definitive Mx : Oopherectomy
indications :
1. Technical difficulties due to increased
vascularity & fragility
2. Rarely profuse/uncontrolled hemorrhage
42. Cervical Ectopic Pregnancy
• Rare, less than 1% of all ectopic gestations
• Have an estimated incidence of one in 2500 to
one in 18,000 pregnancies.
• Passage of a blastocyst through the uterine
cavity and its subsequent implantation and
growth within the mucosa that lines the
endocervical canal
• Dx frequently delayed and is often made
intraoperatively in the presence of extensive
hemorrhage, necessitating an emergency
hysterectomy in about 50% of cases
43. The Aetiology is unknown,
• likely to result from a combination of factors
including local cervical pathology.
• Predisposing factors include
• previous instrumentation
• anatomic anomalies (myomas, synechiae),
• Intrauterine device (IUD) use,
• in vitro fertilisation (IVF 3.7%), and
• diethylstilbestrol exposure, although these are
not strong associations.
44. Presentation
• Presenting symptoms generally include
• Vaginal bleeding which is usually painless but
may be coupled with
• Abdominal pain and urinary problems,
particularly in more advanced pregnancies
• Examination findings at admission vary,
• Enlarged, Globular or
• Distended cervix, which is often associated with
dilatation of the external os.
45. Rubin's criteria Dx cv preg
• close attachment of the placenta to the cervix,
cervical glands present opposite the
implantation site,
• placental location below uterine vessel
insertion or below anterior and posterior
reflections of the visceral peritoneum of the
uterus, and
• No fetal elements in the uterine corpus
46. Clinical criteria
• Uterine bleeding without cramping pain following
a period of amenorrhea
• A soft, enlarged cervix equal to or larger than the
fundus
• The presence of a closed internal os,
• No chorionic tissue found on curettage of the
endometrial cavity, and
• Dilation of the external os
47.
48.
49. DDX
• A cervical ectopic pregnancy and
• Intrauterine pregnancies with a low
implantation site (isthmico-cervical
pregnancy) or in the process of spontaneous
expulsion
• Incomplete Abortion
50. …DDX
• cardiac activity is often seen in a cervical
pregnancy with a visible embryo, but not in an
incomplete abortion
• the gestational sac of a cervical pregnancy has
regular contours, while an incomplete abortion
sac often has irregular contours that may change
shape during the scan
• the cervical os is typically closed in a cervical
pregnancy, but is open in an incomplete abortion
51. MX
• In the past hysterectomy often performed
• A range of conservative (uterus preserving)
treatment options have been suggested and may
be broadly categorised as:
• Cerclage
• Curettage and tamponade,
• Reduction of blood supply, Arterial Embolization
• Excision of trophoblastic tissue,
• intra amniotic fetocide and systemic chemotherapy
(Medical Management)
52. …cnt’d
• Dilatation and curettage, with uterine artery
ligation or embolisation, or cervical balloon
tamponade to prevent blood loss
– had a high failure rate (hysterectomy required in
22% of patients)
– their role is now limited mainly to patients with
life-threatening bleeding
53. …cnt’d
• Local injection of the ectopic pregnancy with
potassium chloride or methotrexate became
the favoured technique in the late 1990s.
• The success rates were high (close to 100%)
• Systemic side-effects and complication rates
low
54. Heterotopic Pregnancy
• Coexistence of an IUP & ectopic pregnancy.
• The incidence is estimated to be 1: 30,000 of
spontaneous pregnancy.
• With the use of ovulation induction & ART, the incidence
is higher.
• Potentially a fatal condition, because
• diagnosis is often missed
• 50 % of cases present late with rupture
• associated with profuse hemorrhage
55. …cnt’d
Diagnosis : Criteria that aid diagnosis
• Uterine size compatible or more with date
• With persistent or rising β-hCG after D & C or
spontaneous abortion
• Presence of two corpus luteum
• Absence of vaginal bleeding with sign &
symptoms of an ectopic pregnancy
• After ART
• Ultrasonographic evidence of IUP & extra
uterine pregnancy
56. …cnt’d
Management.
• Systemic MTX is contraindicated in the presence of
IUP.
• LAPAROSCOPY: 60 % of patients with viable IUP at
the time of surgery had favorable outcome.
• LAPAROTOMY: Indicated in patients with
• hermodynamically unstable
• an interstitial- IUP is present
• Local injection of KCl into the extra uterine
gestation
57. cesarean scar ectopic pregnancy (CSP)
• Pregnancy implanted in a cesarean section
scar
• Rarest forms of ectopic pregnancy, 6 percent
of ectopic pregnancies among women with a
prior cesarean delivery
• Increased report
• Increase in c/s rate
• Better diagnostic accuracy of this condition
58. Strict imaging criteria to establish the
diagnosis:
• Empty uterus,
• Empty cervical canal,
• Development of the sac
in the anterior part of
isthmic portion, and
• A diminished
myometrial layer
between the bladder
and the sac
59. Management
• wedge resection of the ectopic pregnancy via
laparotomy or laparoscopy
• Hysteroscopic excision
• remove the pregnancy and repair the defect
• Local injection of 5 mEq KCl into the sac, and
• Local or systemic MTX administration
• risk of rupture and hemorrhage; hysterectomy may be
necessary
• Expectant management is not a good option
because of the risk of rupture and maternal death
• Recurrence, uterine rupture, placenta accreta,
severe hemorrhage in subsequent pregnancy
60. Pregnancies of unknown location(PUL)
• when a woman has a positive pregnancy test,
but no pregnancy can be visualised on
transvaginal ultrasound (TVS).
• low PUL rates of 7–10%, some report 30%
• modern units should try to maintain a PUL
rate of less than 15%
62. MX
• Expectant management has been shown to be
safe for the majority of women.
• Serum progesterone levels have been used to
predict the outcome of PULs, but appear better
at predicting pregnancy viability than pregnancy
location.
• The change in serum hCG over 48 hours
expressed as the hCG ratio (hCG 48 hours/hCG 0
hours) is helpful in predicting the outcome of
PULs.
• Diagnostic laparoscopy or uterine curettage
should not be undertaken routinely
63. References
• JohnA.Rock, Howard W.jones, Ectopic Pregnancy TeLinde’s operative
Gynecology 10th edition
• Cunningham,Leveno, Bloom, Hauth, Rouse, Spong, Ectopic
Pregnancy , Williams Obstetrics 23rd Edition
• Prof. Lukman Yusuf , lecture note on Ectopic pregnancy
• MARTIN G. SHELTON, THE TREATMENT OF ABDOMINAL PREGNANCIES,
S.A. MEDICAL JOURNA L, 1 June 1963
• Dahab et al. Journal of Medical Case Reports 2011, Full-term extrauterine
abdominal pregnancy: a case report,
http://www.jmedicalcasereports.com/content/5/1/531
• Geneviève et al. , Imaging in the Management of Abdominal Pregnancy: A
Case Report and Review of the Literature, JANUARY JOGC JANVIER 2009
• Nuru Abseno, workineh Getaneh,Cases of Advanced Abdominal
pregnancies one of which was with viable fetus, Ethiop Med J, 42 2004
64. …cnt’d
• Thomas A Molinaro Kurt T Barnhart, Abdominal pregnancy,
cesarean scar pregnancy, and heterotopic pregnancy, UpToDate
19.1
• E. Kirk et al. Pregnancies of unknown location, Best Practice & Research
Clinical Obstetrics and Gynaecology 23 (2009) 493–499
• P. M. Lam et al. Unsuccessful medical treatment of cesarean scar ectopic
pregnancy with systemic methotrexate: a report of two cases, Acta Obstet
Gynecol Scand 2004: 83: 108--116
• A. Nassar et al. Cervical pregnancy after in vitro fertilization and embryo
transfer successfully treated with methotrexate and intracervical injection
of vasopressin, Acta Obstet Gynecol Scand 2004; 83: 112–114
• F. USIFO, S. THAMBAN, I. O. OPEMUYI, & S. SAHOO, Ovarian ectopic
pregnancy, Gynaecology case reports, J Obstet Gynaecol ,
www.informahealthcare.com, accessed 06/16/12
• SAMUEL LURIE,DAVID RABINERSOAN AND, ZEEVS HOHAM, The veracious
etiology of ectopic pregnancy, Acta Obstet Gynecol Scand 1998; 77: 120-
121, www.informahealthcare.com
65. …cnt’d
• J. O. AMAGADA and S. J. VINE, Spontaneous heterotopic pregnancy
remains a diagnostic enigma, Obstetric case reports, J Obstet
Gynaecol www.informahealthcare.com
• N. Acheson et al, Advanced abdominal pregnancy: difficulties in
diagnosis, Journal of Obstetrics and Gynaecology (1996) Vol. 16,
235-238, www.informahealthcare.com
• Radwan Faraj / Martin Steel, Review Management of cornual
(interstitial) pregnancy, Royal College of Obstetricians and
Gynaecologists 2007; 9:249–255, www.rcog.org.uk/togonline,
• Getahun kifle, An abdominal pregnancy with infected gestational
sac , 1987.ethiop. Med. J. 25,41
• Novak
ultrasonic criteria were developed by (Raskin, 1978; Hofmann et al., 1987)
The differential diagnosis initially must include cervical cancer, presence of a cervical fibroid, trophoblastic tumor, and
abnormalities of placental location such as a placenta previa or low-lying placenta