Download as PDF, PPTX






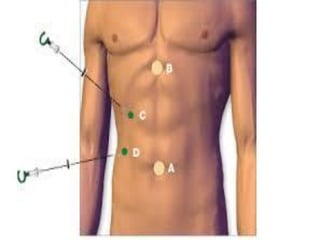





This document compares open and laparoscopic cholecystectomy procedures. Open cholecystectomy is easier to perform and more cost effective, but results in a longer hospital stay and poorer cosmetic outcomes. Laparoscopic cholecystectomy is now the gold standard, providing shorter recovery time and fewer complications, but requires specialized equipment and training and carries a higher risk of duct injuries. Both approaches are appropriate depending on the patient's condition and surgeon's expertise.





























































![16.4 Operative surgery Gallbladder and appendix [Autosaved] [Autosaved] [Auto...](https://cdn.slidesharecdn.com/ss_thumbnails/16-250116203957-9e9d1712-thumbnail.jpg?width=640&height=640&fit=bounds)





























![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















