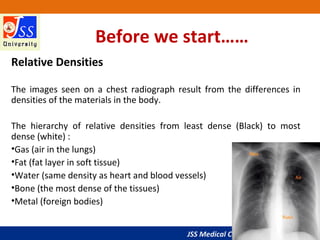
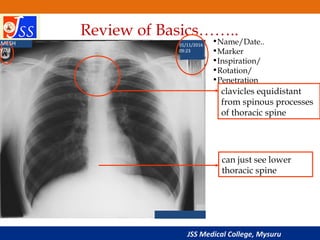
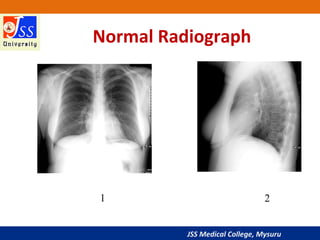
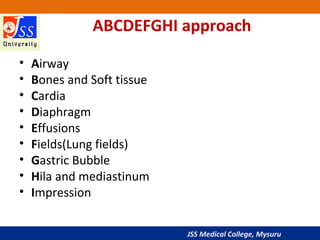
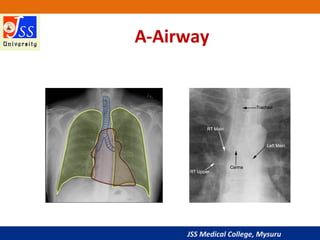
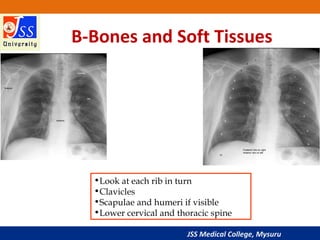
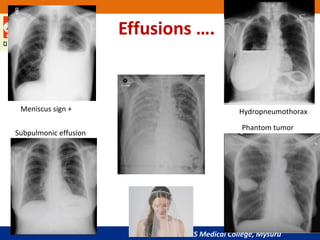
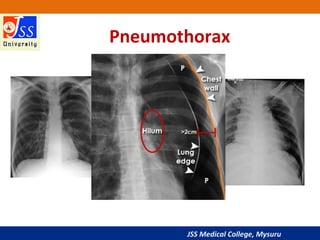
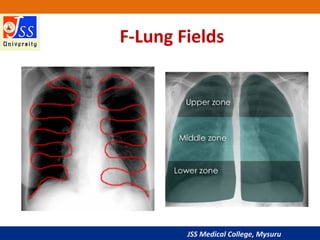
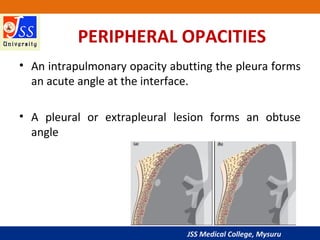
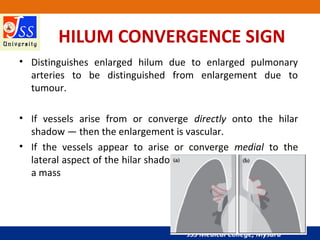
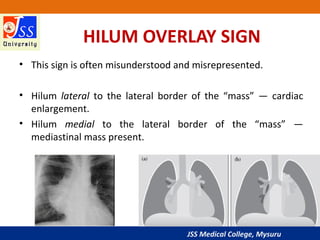
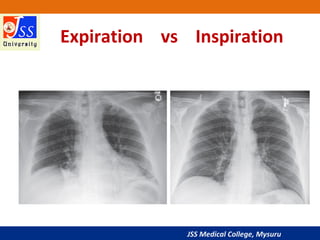
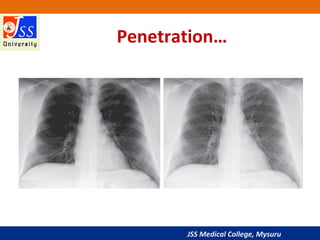
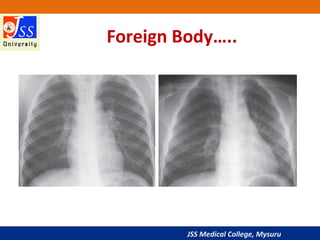
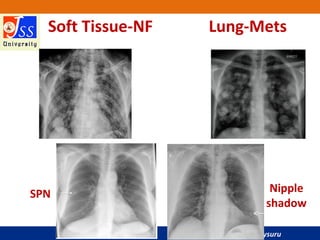
This document provides a comprehensive overview of chest X-ray interpretation, emphasizing the importance of understanding what a normal chest X-ray looks like in order to identify abnormalities. Key principles include having a systematic approach, interpreting findings in conjunction with clinical information, and recognizing specific technical factors such as inspiration, penetration, and rotation. Various X-ray views and assessments, including methods for identifying pleural effusions and analyzing lung fields, hila, and mediastinum, are also discussed.