Downloaded 351 times
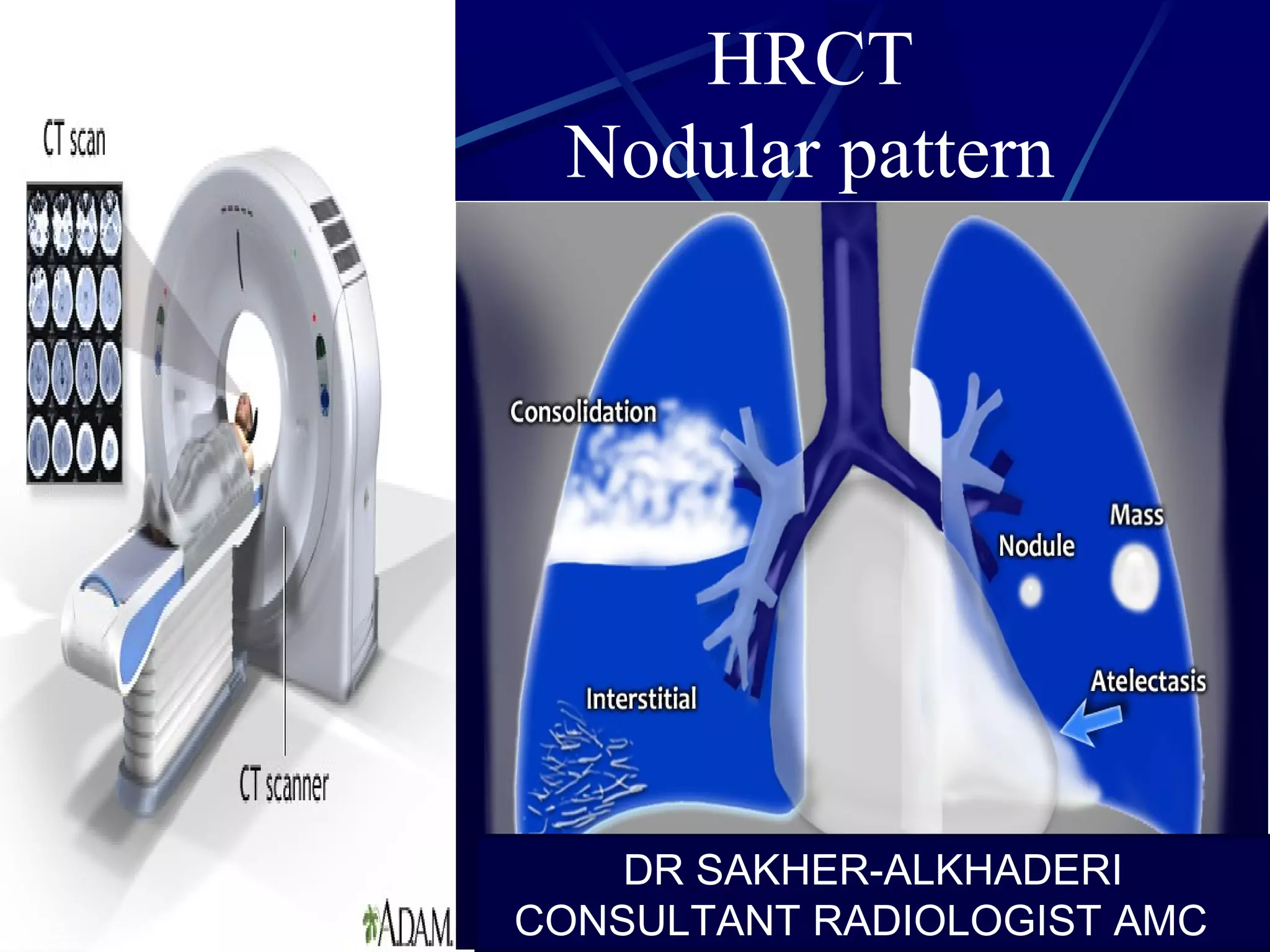
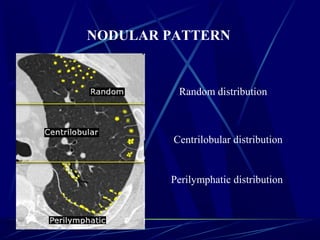
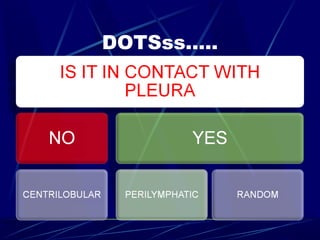
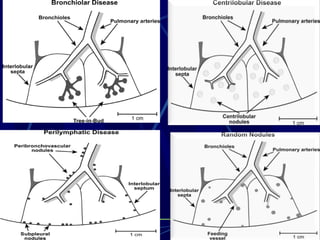
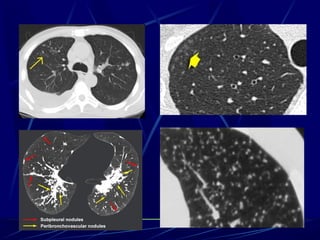
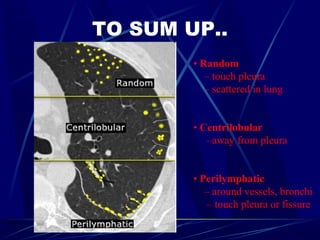
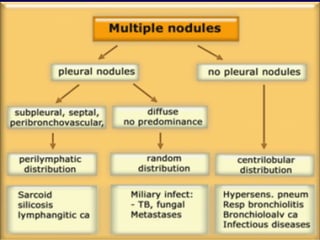
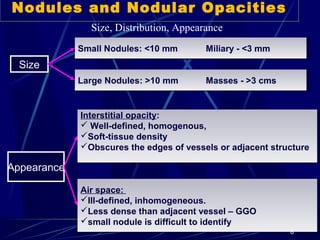
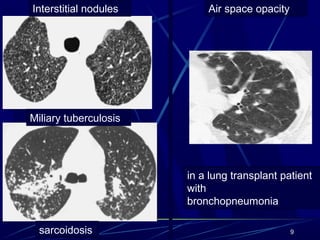
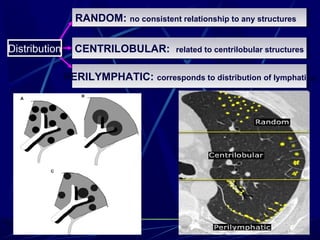
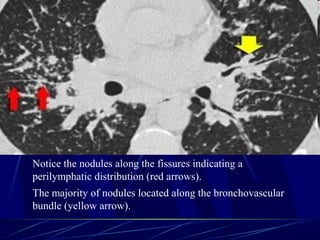
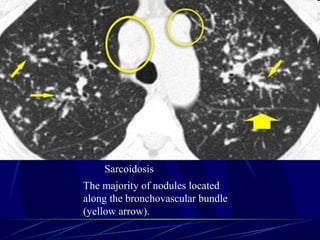
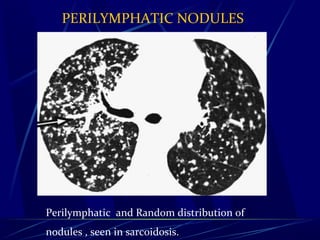


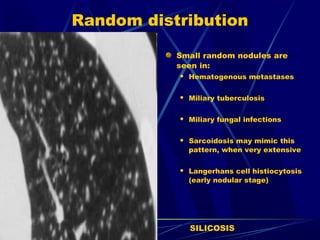
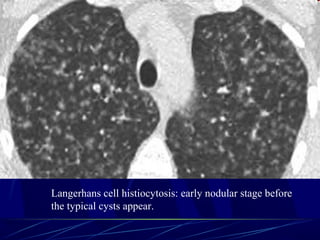
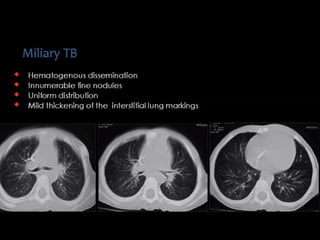
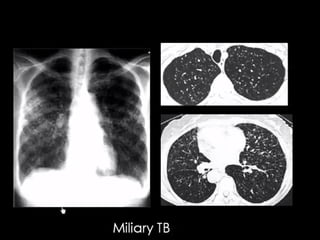
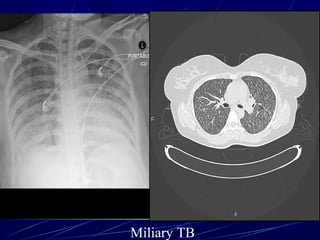
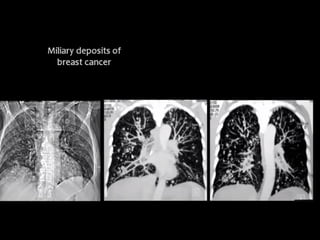
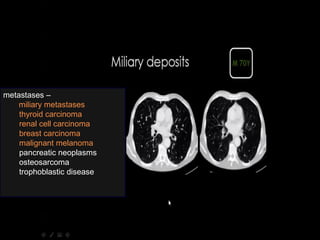

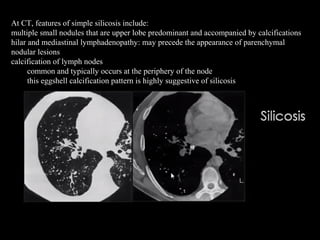
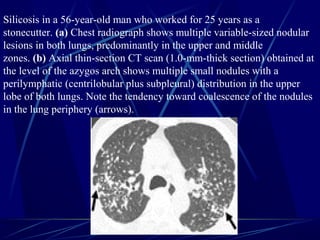
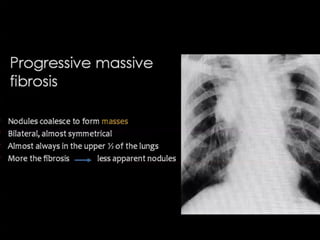
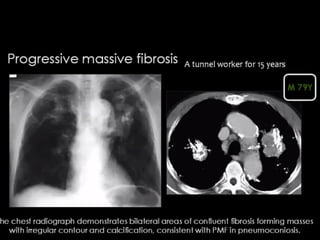
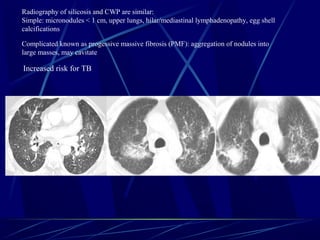
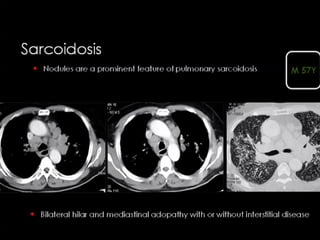


The document discusses the HRCT nodular patterns in the lungs, categorizing them into random, centrilobular, and perilymphatic distributions, with specific focus on size and appearance of nodules. It details conditions such as sarcoidosis and hypersensitivity pneumonitis, including various occupational lung diseases and their radiographic characteristics. The document also highlights the presentation of miliary tuberculosis and silicosis, describing typical findings on chest imaging.
















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
