Downloaded 381 times
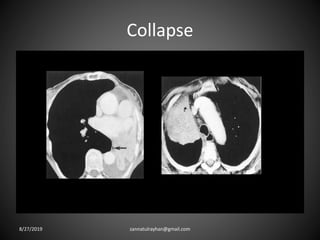
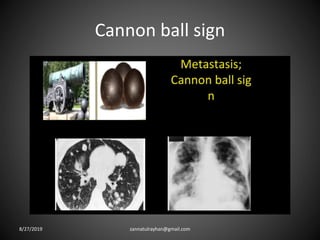
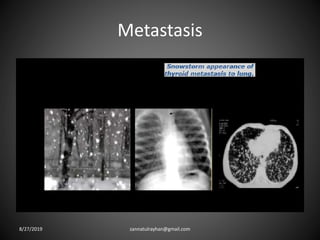
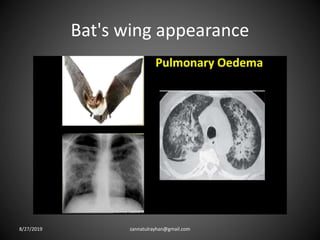
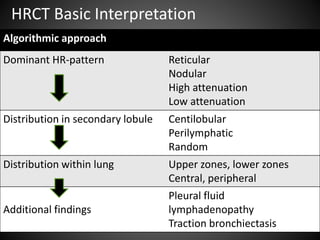
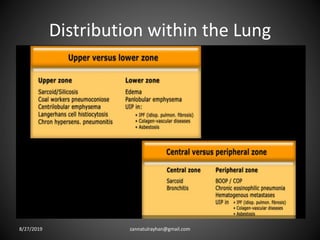

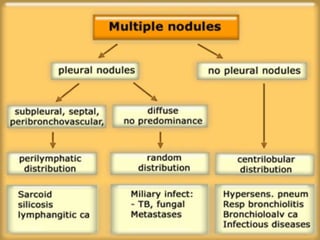
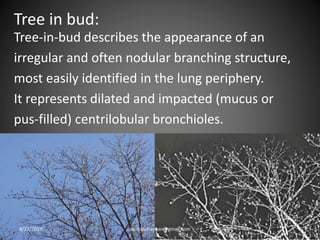
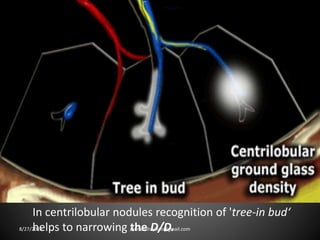
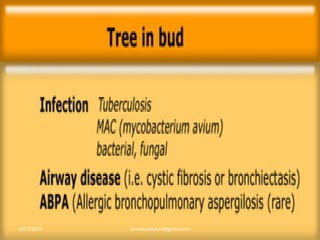
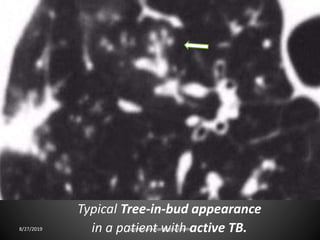
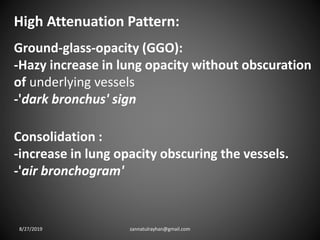
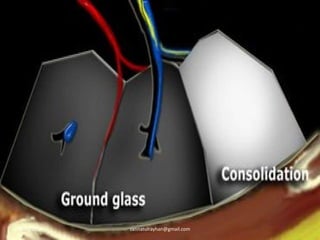
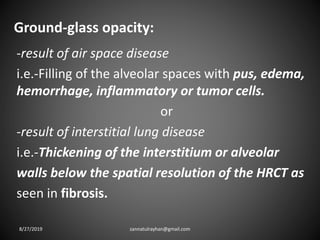
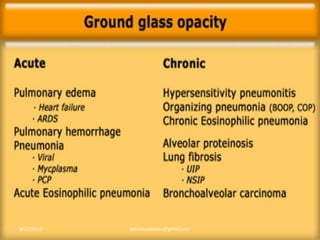
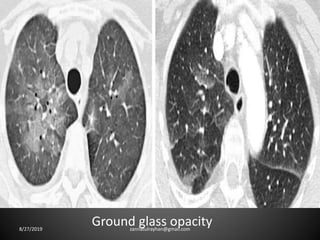
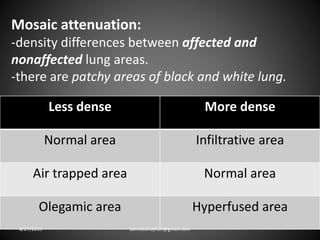
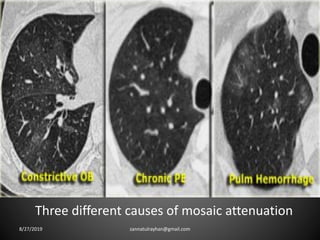
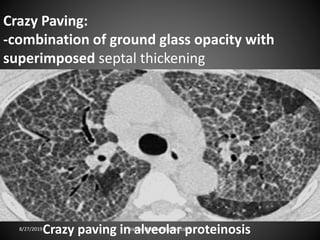
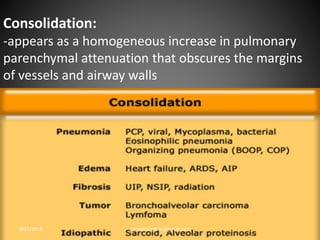

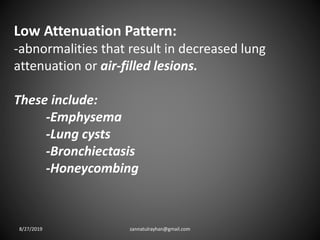
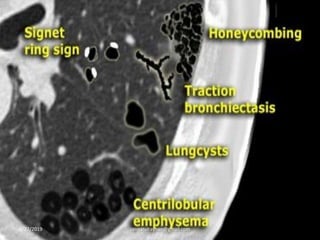




This document provides an overview of CT chest imaging, including standard CT, high-resolution CT, and their indications. It discusses CT chest anatomy and windows. Common lung pathologies seen on standard CT like bronchial carcinoma, collapse, and metastasis are described. Interpretation of high-resolution CT focuses on patterns such as reticular, nodular, ground glass opacity, and consolidation. Specific findings including honeycombing, tree-in-bud, mosaic attenuation, and crazy paving are explained. The document concludes with a discussion of low attenuation patterns including emphysema, lung cysts, and bronchiectasis.





























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









