This document discusses the surgical management of neurogenic bladder through various procedures like neuromodulation, augmentation enterocystoplasty, and denervation procedures. It provides details on electrical stimulation techniques for both storage and voiding disorders in neurogenic bladder. These include transurethral electrical bladder stimulation, sacral rhizotomy, and sacral neuromodulation. The document outlines patient selection criteria and techniques for sacral neuromodulation, including a two-stage process of temporary lead placement and permanent implantable pulse generator implantation. Putative mechanisms of action and expanding clinical indications for sacral neuromodulation are also discussed.


![Treatment Detrusor overactivity
Neuromodulation
Augmentation enterocystoplasty[*]
Autoaugmentation[*]
Denervation procedures
Urinary diversion
Low bladder compliance
Augmentation enterocystoplasty[*]
Autoaugmentation[*]
Denervation Procedures
Sphincteric dysfunction
Surgery
Midurethral sling
Pubovaginal sling
Urethral/colposuspension
Artificial urinary sphincter
3 Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/bladder-neurogenic-management-surgical-converted-210611155306/75/Bladder-neurogenic-management-surgical-3-2048.jpg)















![Technique
Sacral nerve stimulation (SNS) by the InterStim[*]
procedure is performed in two stages:
Stage I, a clinical trial of a temporary or
permanent lead for external stimulation; and
Stage II, implantation of a subcutaneous
implantable pulse generator (IPG).
Each stage can be performed with monitored
anesthesia care supplemented by local anesthesia.
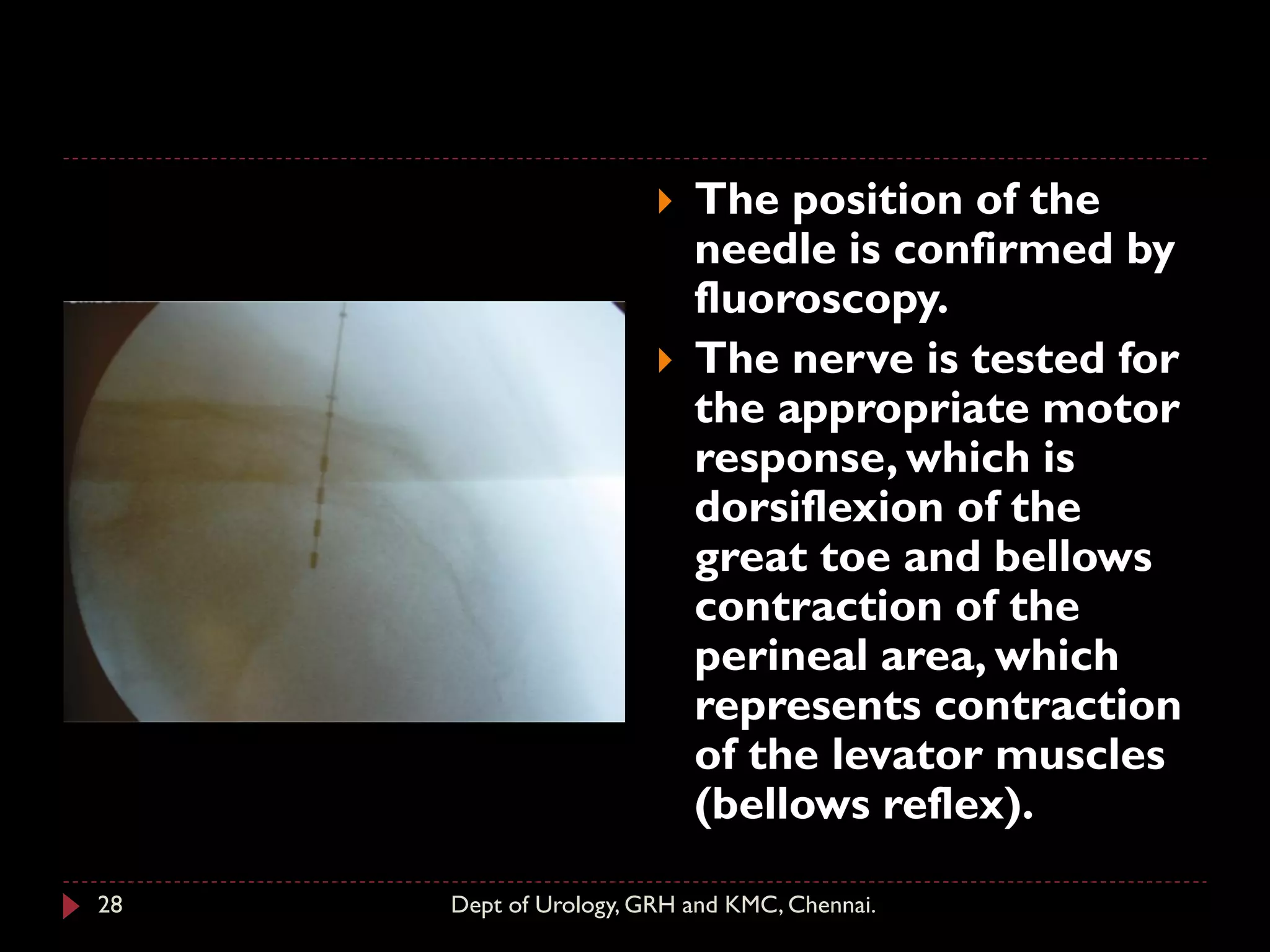
During the initial introduction of sacral
neuromodulation therapy, patients underwent a
percutaneous nerve evaluation by the placement
of a unilateral percutaneous lead in the S3
foramen with use of local injectable anesthesia.
22 Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/bladder-neurogenic-management-surgical-converted-210611155306/75/Bladder-neurogenic-management-surgical-22-2048.jpg)









![Selective Nerve Stimulation
Pudendal Nerve
The Bion device[*] is a minimally invasive
implantable ministimulator with an integrated
electrode for nerve neuromodulation.
Early feasibility trial results of the Bion device
placed at the level of the pudendal nerve exiting
Alcock's canal indicate that a considerable
reduction in the degree of detrusor overactivity
incontinence can be obtained in refractory cases,
including those cases of failed SNS
neuromodulation ( Bosch, 2005 ).
Clinical trials of the rechargeable Bion device are
under way in the United States and Europe.
36 Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/bladder-neurogenic-management-surgical-converted-210611155306/75/Bladder-neurogenic-management-surgical-36-2048.jpg)

![ Stimulation of the dorsal penile nerve has been tested
in humans to control incontinence in individuals with
spinal cord injury and increase bladder volume and
reduce bladder overactivity
Electrical stimulation of the dorsal genital nerves can
abolish detrusor overactivity and increase bladder
capacity in individuals with neurogenic detrusor
overactivity due to spinal injury.
Feasibility trials with MEDStim,[*] an implantable
neuroelectrode and pulse generator, are under way to
determine the optimal stimulation parameters that
have limited its application in the past for increasing
bladder capacity and treating the symptoms of
idiopathic detrusor overactivity in otherwise healthy
persons.
38 Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/bladder-neurogenic-management-surgical-converted-210611155306/75/Bladder-neurogenic-management-surgical-38-2048.jpg)
![Posterior Tibial Nerve
The posterior tibial nerve is a mixed sensory and motor nerve
containing fibers originating from spinal roots L4 through S3 that
modulate the somatic and autonomic nerves to the pelvic floor muscles,
bladder, and urinary sphincter.
On the basis of translational findings of the traditional Chinese practice
of using acupuncture points over the common peroneal or posterior
tibial nerve to inhibit bladder activity,
McGuire and associates (1983) used transcutaneous stimulation of the
common peroneal or posterior tibial nerve for inhibition of detrusor
overactivity.
PTNS[†] as approved by the FDA currently consists of weekly 30-minute
stimulation treatments provided by insertion of a small-gauge
stimulating needle approximately 5 cm cephalad from the medial
malleolus and just posterior to the margin of the tibia with the
grounding electrode pad placed on the medial surface of the calcaneus
PTNS is minimally invasive, demonstrates efficacy, and is easily applicable
and well tolerated in all the lower urinary tract conditions studied.
39 Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/bladder-neurogenic-management-surgical-converted-210611155306/75/Bladder-neurogenic-management-surgical-39-2048.jpg)