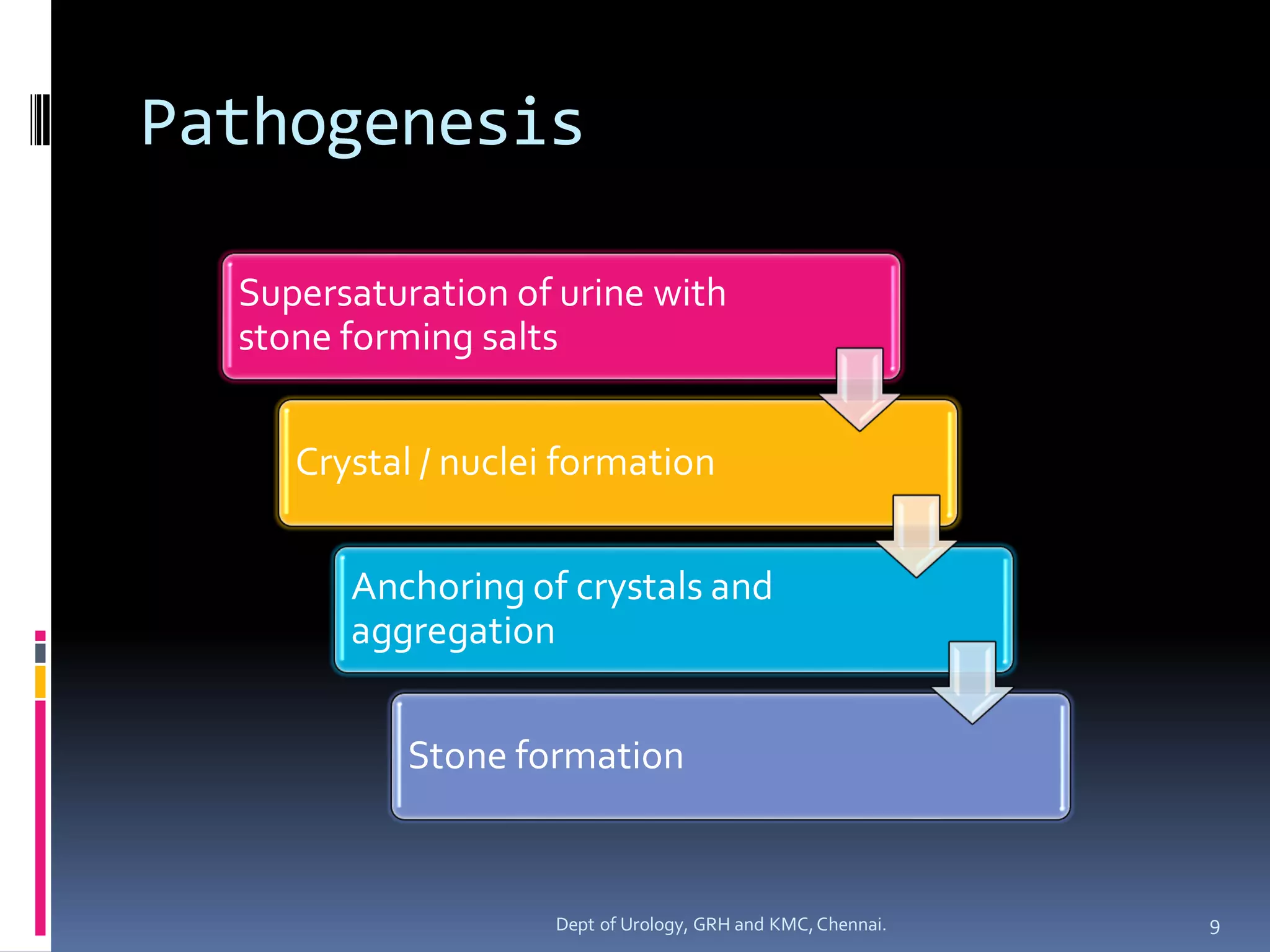
The document discusses the etiopathogenesis of urolithiasis or kidney stone formation. It covers topics like epidemiology, risk factors related to gender, age, geography, occupation and diet. It then describes the pathophysiological processes involved - supersaturation of urine, crystal nucleation, growth and aggregation. It discusses theories around crystal fixation and Randall's plaques. Various inhibitors that prevent stone formation are also outlined. The role of the non-crystalline matrix component of stones is briefly mentioned.