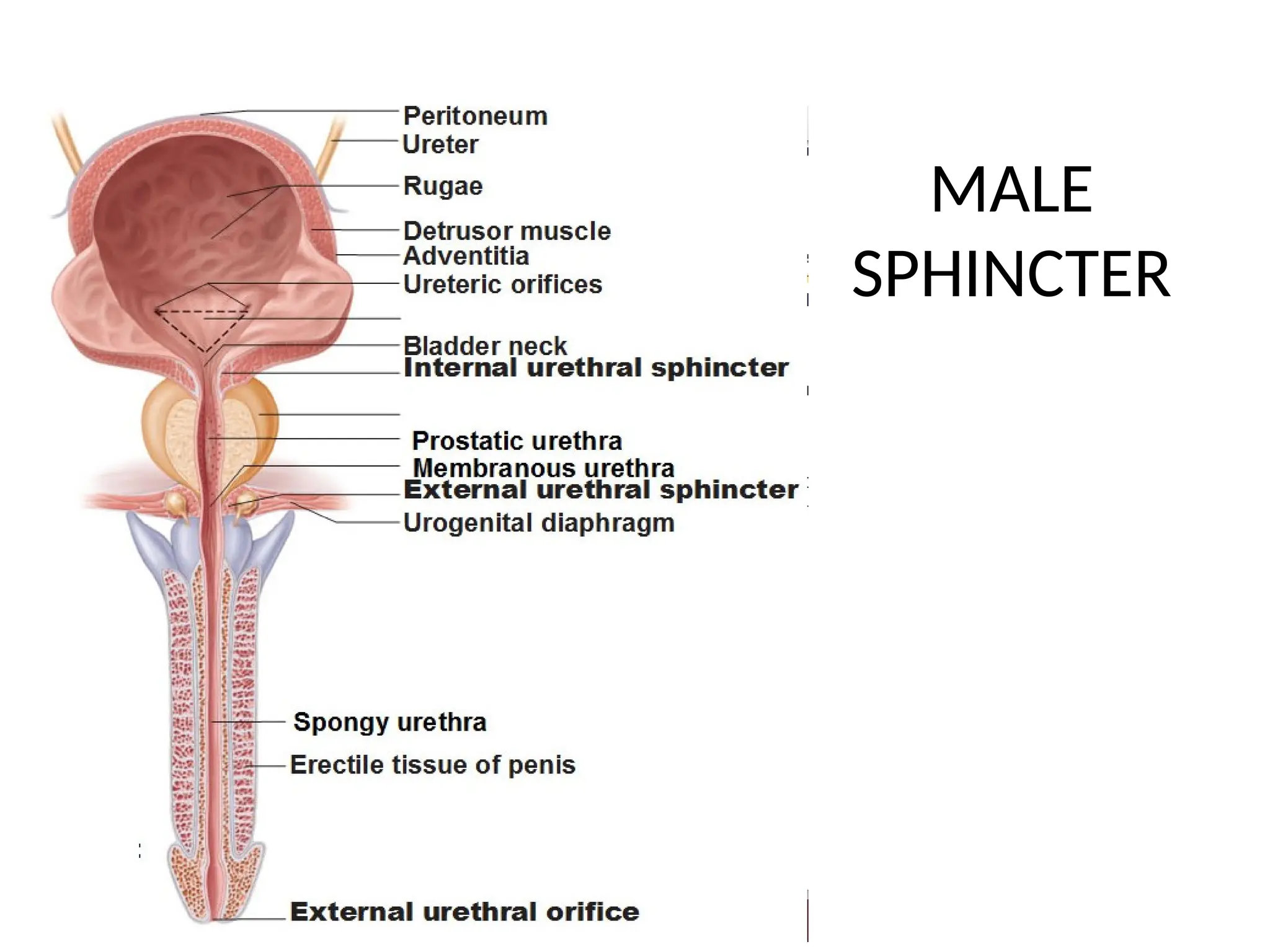
Male Sphincter Anatomy
1.Internal Urethral Sphincter:
Made of smooth muscle, controlled by the autonomic nervous system
2. External Urethral Sphincter:
Made of skeletal muscle and under voluntary control.
Female Sphincter Anatomy
1.Internal Urethral Sphincter:
Located at the bladder neck, though it lacks a specific anatomical structure.
2. External Urethral Sphincter:
Similar in structure and function to the male external sphincter.
Why we needinnervation for bladder?
• Urine is produced at 0.3 ml/ sec. but emptying
is intermittent. So urine has to be stored.
• It has to be under low pressure to prevent
reflux.
• It has to be co ordinated between body and
base.
12.
Structures involved
• Bladderwall receptors
• Sacral center
• Afferent and efferent nerves
• External sphincter (pudendal nerve)
• Intermediolateral grey sympathetic chain
• The periaqueductal gray (PAG)
• Barrington’s nucleus
• Paracentral lobule and prefrontal regions
Cortical Centers forMicturition
• Frontal Lobe
• Send tonically inhibitory signals to the detrusor
muscle to prevent the bladder from emptying
(contracting) until a socially acceptable time and
place to urinate is available.
19.
Pontine Micturition Centre
•Barrington’s Nucleus
• Dorsomedial tegmental region – center for micturition (M-
region).
• Ventrolateral pontine tegmentum – center for storage (L-
region).
• Pontomesencephalic reticular formation
• Mediated by reticulospinal tracts which synapse with detrusor
and sphincter motor center in sacral cord
INNERVATIO
N TYPE
ORIGIN NERVEPOST-GANGLIONIC
FIBRES
FUNCTION
SYMPATHETI
C
T11-L2
↓
Synapse with
Inferior
Mesenteric/
Hypogastric
plexus
HYPOGASTR
IC NERVE
α –Bladder neck/proximal
urethra(contraction)
β-Bladder fundus-
relaxation
Inhibits Parasympathetic
Ganglia in Detrusor wall
STORAGE
PARASYMPAT
HETIC
S2-4
(DETRUSOR
NUCLEUS)
PELVIC
NERVE
M2,M3(Ach)-Detrusor
contraction
Proximal urethra(NO)-IUS
relaxation
VOIDING
SOMATIC
(to EUS)
S2-4
(PUDENDAL
NUCLEUS)
PUDENDAL
NERVE
Conscious state-
supraspinal centres
activate Pudendal Nu-
keeps EUS tonically
contracted
VOLUNTAR
CONTROL
22.
Afferent System
• Pelvic(mostly),hypogastric and pudendal nerves.
• spinal sensory pathway (need to urinate, pain, temperature,
urgency )-anterolateral column
• conscious sensitivity (bladder distention, ongoing micturition,
and tactile pressure) –posterior column
• Afferents-
1. myelinated Aδ fibers (low-threshold afferents)
2. unmyelinated C fibers /silent fibres-(high-threshold afferents)
23.
NEUROGENIC BLADDER: DEFINITION
•Refersto dysfunction of urinary bladder due to
disease of CNS or peripheral nerves involved in the
control of micturition.
24.
NEUROGENIC BLADDER: CAUSES
1.Central Nervous System Disorders:
Stroke:
Parkinson’s Disease:
Multiple Sclerosis (MS):
2. Spinal Cord Injury:
Trauma or Accidents:
Spina Bifida:
3. Peripheral Nerve Damage:
Diabetes:
Pelvic Surgery or Trauma:
4. Other Neurological Conditions:
Cerebral Palsy:
Tumors or Cysts:
25.
Physiology
• More than100 ml of urine accumulated- bladder
wall receptor are facilitated
• Thereby default relax the body and contract the
sphincter
• At 300 ml the afferent roots and nerves carry
impulses to sacral centre which caries the sense
of fullness through posterior column
• When overdistended- pain through spino-
thalamic tract
26.
• At barringtoncenter and PAG-low pressure filling
can be maintained upto 450-600ml
• Beyond 600ml if urine not emptied-impulses are
transmitted to paracentral areas for facilitation and
prefrontal for inhibition
• Based on social situation bladder can be distended
upto 1.5-2 litre
27.
• Efferent areboth facilitatory and inhibitory and
travel via spinal cord tracts and participate in
functional Bradley's loop
• When facilitation is planned by cortical centre,
internal sphincter opens and urine trickles in
proximal urethra and that becomes stimulus for
sacral parasympathetic- contract body and relax
sphincter
• Voluntary activation of Onuf nucleus and
pudendal nerve- external sphincter opens
28.
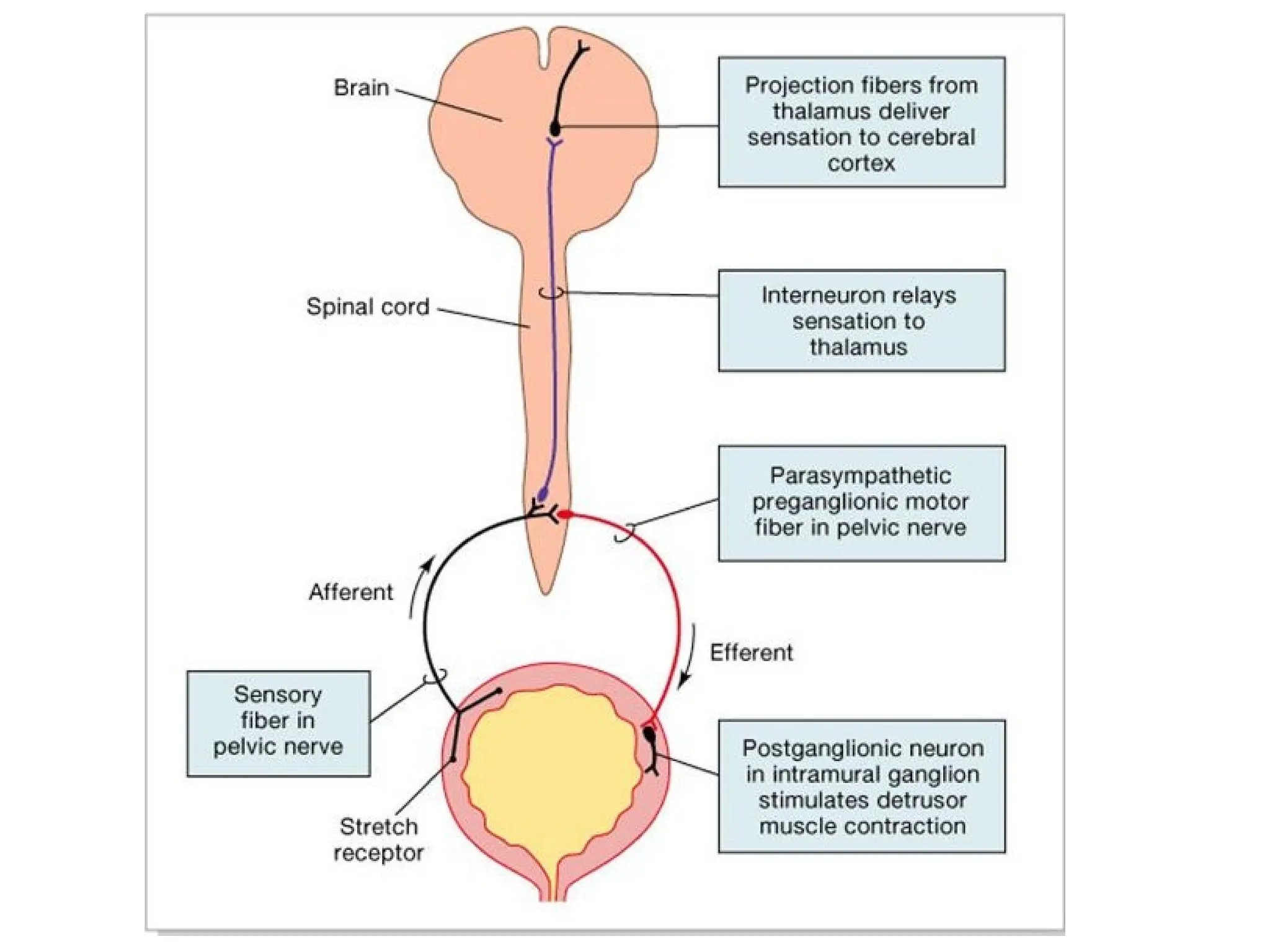
Micturition Reflex
• Sensorysignals from the bladder stretch receptors are
conducted to the sacral segments of the cord through the pelvic
nerves and then reflexively back again to the bladder through
the parasympathetic nerve fibers by way of these same nerves.
• Sacral reflex center is the primitive voiding center in infants.
• Ability of the brain to control the PMC is part of the social
training that children experience during growth(18m -3y)
31.
PHASES
• Micturition isconsidered as having two phases:
• the filling (storage) phase and
• the emptying (voiding) phase.
• Sacral Voiding Centre- Conus medullaris
32.
• Storage phase-
•No neural bladder control
needed to store.
• Storage in the face of
distension or pain requires
neural inhibition of voiding.
• Voiding phase-
• Entirely under neural
control – unlike storage.
• signal to initiate voiding
comes from the bladder, is
okayed by the frontal
cortex, triggered by pons
and executed by sacral cord.
33.
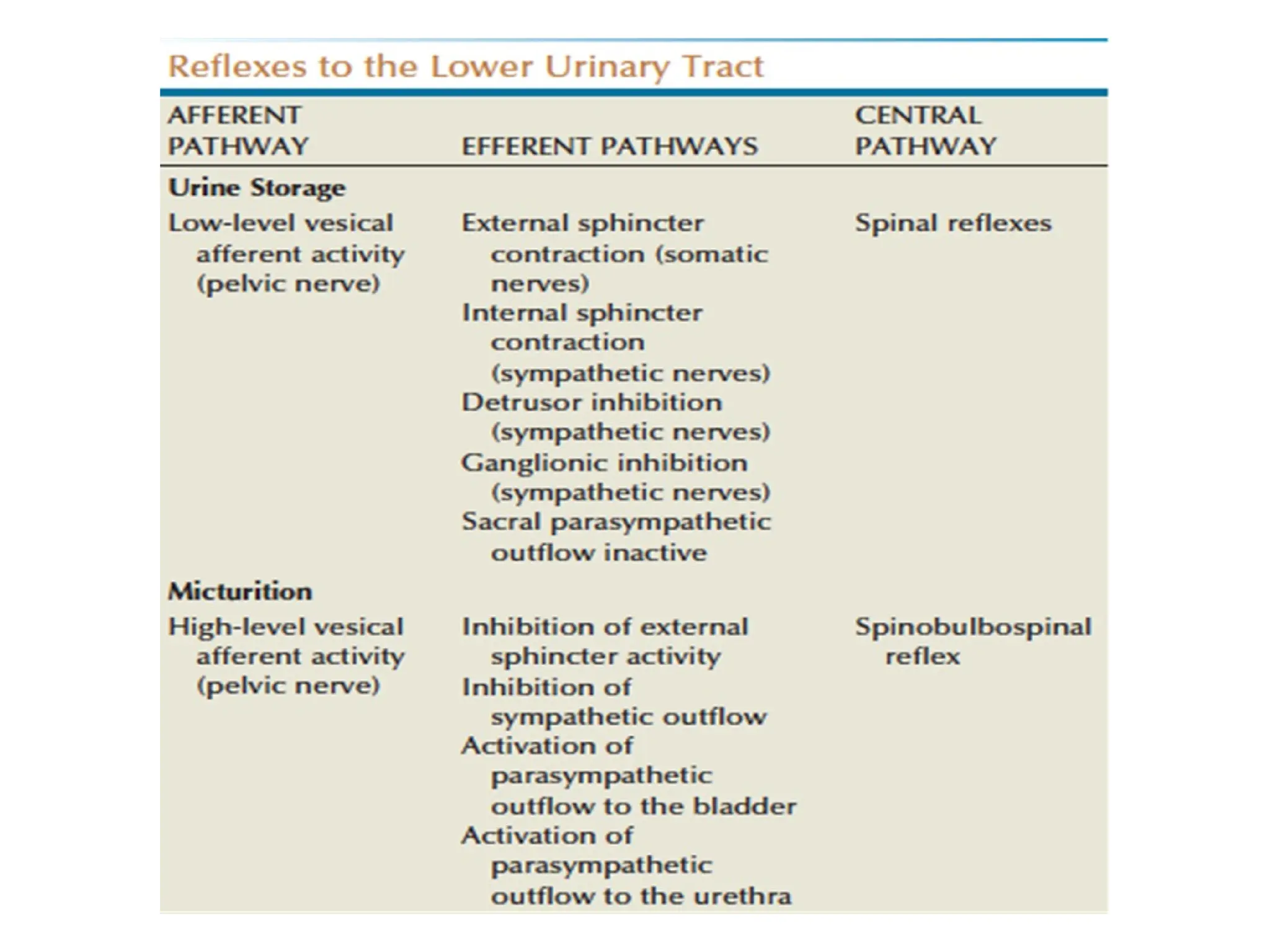
STORAGE PHASE
⮞ Duringstorage , distention of
bladder produces low-level
bladder afferent firing.
⮞ Afferent firing in turn
stimulates the sympathetic
outflow to outlet (base and
urethra) and pudendal outflow
to external urethral sphincter.
⮞ These responses occur by
spinal reflex pathways and
represent “guarding reflexes,”
which promote continence.
⮞ Sympathetic firing also
inhibits detrusor muscle and
transmission in bladder ganglia.
34.
VOIDING PHASE
⮞ Atthe initiation of micturition,
intense vesical afferent activity
activates the PMC, which inhibits the
spinal guarding reflexes.
⮞ The PMC also stimulates the
parasympathetic outflow to the
bladder and internal sphincter smooth
muscle.
⮞ Maintenance of the voiding reflex is
through ascending afferent input
from the spinal cord, which may pass
through the PAG before reaching
PMC.
Uninhibited Neurogenic Bladder
•destructive lesion in the corticoregulatory tracts -- over
facilitation of the micturition reflex.
• frequency, urgency, and urge incontinence
• Urodynamics: normal sensation ,involuntary contraction
at low filling volumes, residual urine is characteristically
low
• patient generally can initiate a bladder contraction
voluntarily but is often unable to do so during cystometry
because sufficient urine storage cannot occur before
involuntary contraction is stimulated
37.
Reflex neurogenic bladder
(AutomaticBladder)
• Interruption between the sacral spinal cord and the brainstem
• No bladder sensation, and there is inability to initiate
voluntary micturition.
• Incontinence without sensation generally results from low-
volume involuntary contraction.
• Striated sphincter dyssynergia is the rule
38.
Sensory Neurogenic Bladder
•Selective interruption of sensory fibers between the bladder
and the spinal cord or the afferent tracts to the brain
• Loss of sensation allows for the bladder to distend without
triggering a reflex bladder contraction.
• Unless voiding is initiated on a timed basis ->varying degrees
of bladder overdistention -> hypotonicity.
• If bladder decompensation occurs -> significant amounts of
residual urine;
• cystometric curve: a large capacity bladder with a flat, high-
compliance, low-pressure filling curve.
39.
Motor Neurogenic Bladder
•Destruction of parasympathetic motor innervation
• normal sensation of bladder filling but is unable to generate
detrusor pressure sufficient to empty the bladder
• Symptoms range from painful urinary retention to only a
relative inability to initiate and maintain normal micturition
• Chronic overdistention and decompensation may occur,
resulting in a large-capacity bladder with a flat, low-pressure
filling curve; a large residual urine may result
40.
Autonomous Neurogenic Bladder
(AtonicBladder)
• Complete motor and sensory separation of the bladder from
the sacral spinal cord
• disease that destroys the sacral cord or causes extensive
damage to the sacral roots or pelvic nerves
• Only bladder wall receptors are there
• Large bladder with no sensation and continuous dribbling
• Low pressure filling and reflux
41.
• Also thetype of dysfunction seen in patients
with spinal shock
• Cystometric pattern is initially similar to the
late stages of the motor or sensory bladder,
with a marked shift to the right of the
cystometric filling curve and a large bladder
capacity at low intra -vesical pressure
42.
UMN/Spastic LMN/Flaccid
• Lesionabove S2
• Urgency, frequency,
urge incontinence
• +/- post voidal residue
• Interrupted flow
• High bladder pressure
• Detrusor Hyperreflexia
with Detrusor sphincter
dyssynergia
• Low bladder capacity
• Lesion below S2
• Hesitancy, Retention
• post voidal residual urine
>100ml
• Poor or absent flow
• Low bladder pressure
• Detrusor Areflexia with
sphincter insufficiency
• High bladder capacity
The International ContinenceSociety classification
system for vesicourethral activity
Neurogenic Voiding Dysfunctions (NVD) Eur Urol
2003; 44/3 (Curric Urol I–XV)
48.
FOUR SCENARIOS
⮚ Goodbladder (compliant), good sphincter
⮚ Good bladder (compliant), bad sphincter
⮚ Bad bladder (low compliance), good sphincter
(innervated, but failing to relax properly)
⮚ Bad bladder (poor compliance), bad sphincter
Neurogenic Voiding Dysfunctions (NVD) Eur
Urol 2003; 44/3 (Curric Urol I–XV)
49.
Evaluation of Bladderdysfunction
• History
• Physical examination
• Laboratory testing
• Imaging studies
• Urodynamic studies
50.
History
• Filling/storage symptomsinclude urinary urgency, frequency
(more than eight voids per 24 hours), incontinence, and
nocturia.
• Voiding symptoms include hesitancy, straining to void,
dysuria, and double voiding.
• Complaints regarding sexual dysfunction.
• Past history of additional medical, neurological, urologic,
obstetric, and gynaecologic problems or surgeries
51.
Physical examination
• Abdominalexamination, inspection of the external genitalia,
and palpation of the flank.
• In men, a digital rectal examination- evaluate prostate
• In women, a vaginal examination
• A complete neurological examination- Bulbocavernous reflex,
anal reflex, perianal sensations and anal tone.
Imaging studies
• LowerUrinary Tract Imaging-
• Cystourethrogram- the presence of vesicoureteral
reflux and the morphologic characteristics of the
bladder, bladder neck, proximal urethra, and striated
sphincter during urine storage, bladder filling, and
voiding
• Direct Visualization by Cystoscopy
• Upper Urinary Tract Imaging-
• Ultrasound- screening modality
• Intravenous Pyelogram, CT, Isotope scans
54.
Urodynamic Studies
• Uroflowmetry
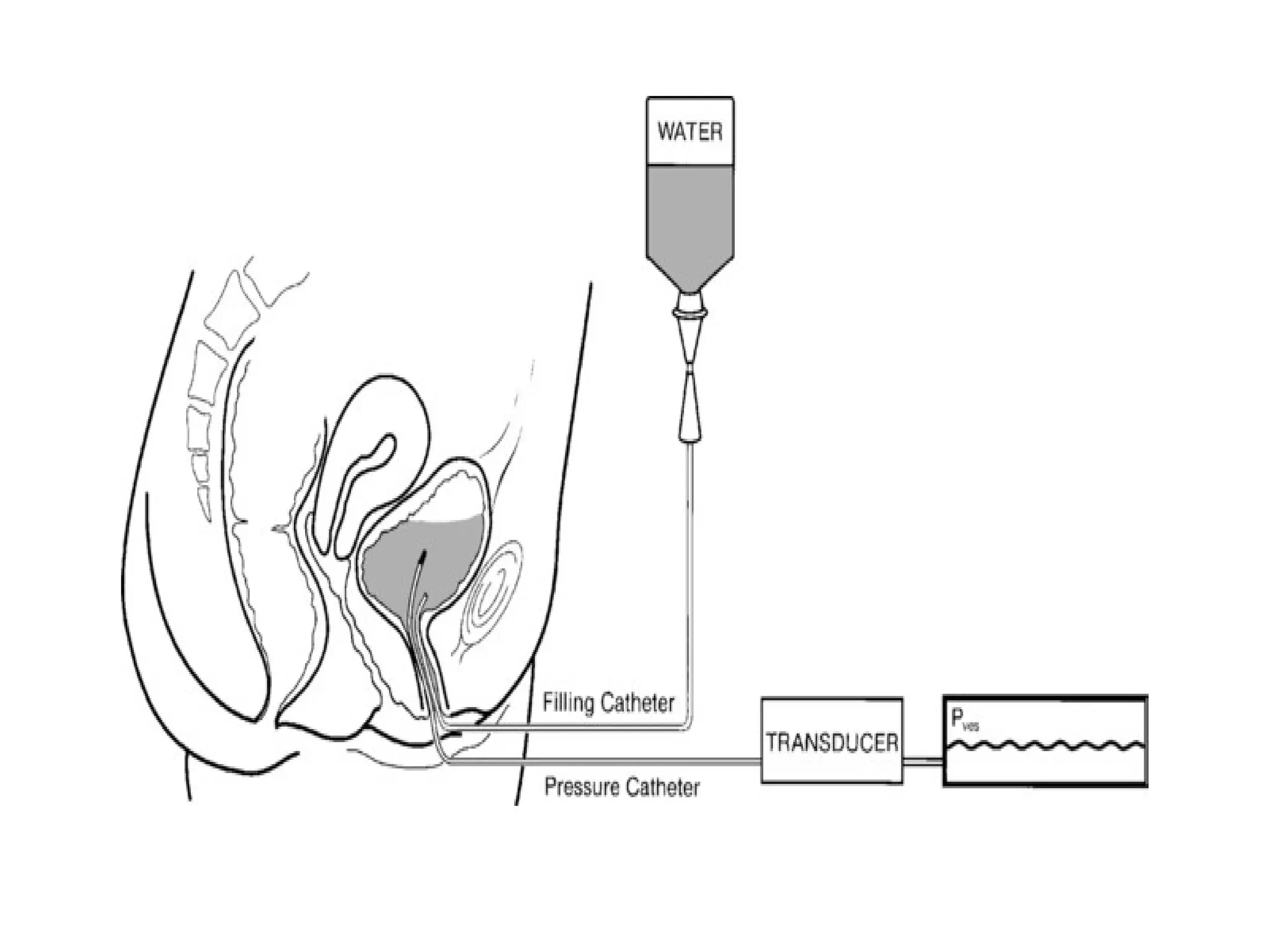
•Filling and Voiding Cystometry
• Electromyography of external sphincter
• Assessment of Post-voidal residual urine
55.
UROFLOWMETRY
• simple non-invasivetest used for measurement of volume of urine
voided per unit time
• Flow depends on two factors—the detrusor contractility and the
urethral resistance.
• The voided volume should be at least 130–150 mL and less than
700 ml to produce accurate curves.
• Young males <40 years : Q max >25 mL/s, and in
females :Q max is 5–10 mL/s more than males at a
given
bladder volume.
59.
Cystometry
• Cystometry isthe measurement of bladder volume and
intravesical pressure during filling and storage phases for the
purpose of evaluating detrusor function. (Bladder Compliance)
• The normal adult volume- 400-750 mL
• maximum bladder pressure of 15 cm water.
• Storage phase-intravesical pressures exceeding 15 cm water
and a steep rising curve in the cystometrogram, possibly due
to bladder inflammation, bladder fibrosis, or detrusor
hypertrophy.
60.
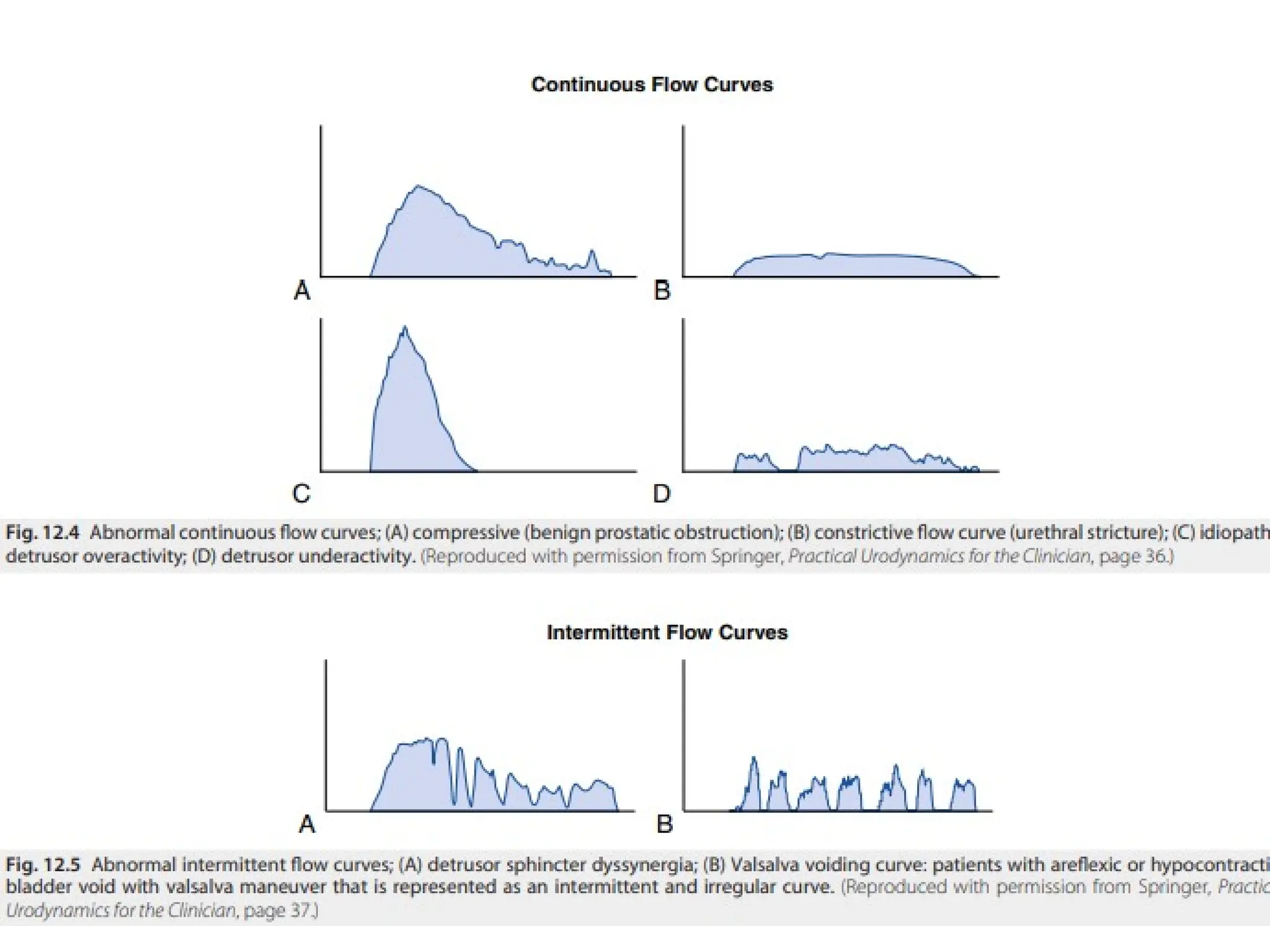
• Voiding phase-Involuntary detrusor contraction (i.e., a phasic
increase in intravesical pressure during the filling phase)
reflects the presence of detrusor hyperreflexia.
• An absence of contractions during attempts to void- areflexic
bladders
62.
Electromyography
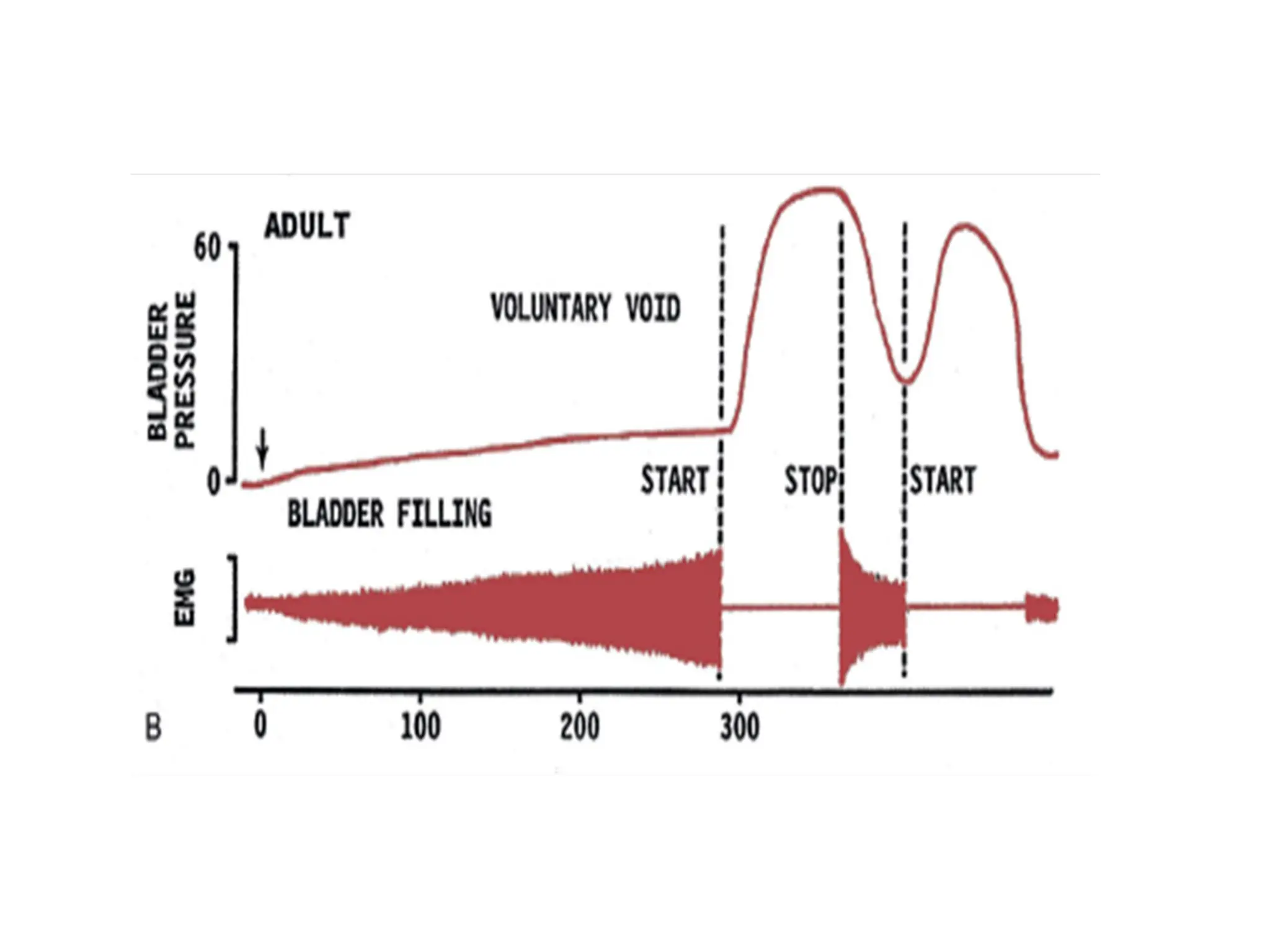
• Sphincter EMG-record bioelectric potentials during bladder
filling, storage, and micturition
• Voluntary control of the pelvic floor musculature and
coordination between the detrusor and pelvic floor.
• During bladder filling, EMG activity should gradually increase
and reach a maximum before voiding.
• True striated sphincter dyssynergia occurs only in patients with
neurological disease or injury at the level of the spinal cord and
represents involuntary sphincter contraction at the time of
detrusor contraction.
• Detrusor-sphincter dyssynergia occurs in patients with
suprasacral SCI and is caused by interruption of the spinobulbar-
spinal pathway that provides coordinated voiding.
#55 poor –detrusor hypoactivity or bladder obstruction
Normal flow depends on age,sex,race
Flow <15 mL/s was generally defined as abnormal in literature, but it is now accepted that absolute flow rates correlate poorly with obstruction
#56 Newborn: bladder capacity= 30 mL; and bladder capacity increasing by about 30 mL each year almost until puberty,
formula (age in years + 1) × 30 = bladder capacity in mL is useful.
Infants= 7 mL/kg.
#58
Common uroflowmetry curves are shown in Figure 11.2. The normal curve is shaped like a bell with Qmax achieved within the initial 1/3rd of voiding time (Fig. 11.2A). Falsely high maximum flow rates may be produced by artifacts (Fig. 11.2B). An intermittent curve (Fig. 11.2C) indicates a straining pattern, which further suggest detrusor underactivity. “Constrictive” obstruction, as in stricture urethra produces a flat, box shaped plateau curve (Fig. 11.2D). “Compressive” obstruction, as in BPH leads to curve with Qmax achieved early in flow, followed by a prolonged tail (Fig. 11.2E).
This test, despite being non-specific, is still widely used because of the sheer simplicity and ease, and also for follow up after treatment of obstruction.























































![Neurogenic bladder [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/neurogenicbladderedmond-140716213757-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)


























