This document provides information about urodynamic evaluation of voiding dysfunction. It discusses the history of urodynamics, aims, equipment used including catheters, flowmeters and EMG equipment. It describes how to conduct urodynamic evaluations including uroflowmetry, cystometrogram, and considerations for filling rate and medium. Key points covered are the indications for urodynamics, preparation of patients, types of equipment and how to interpret uroflow curves and cystometrogram measurements.
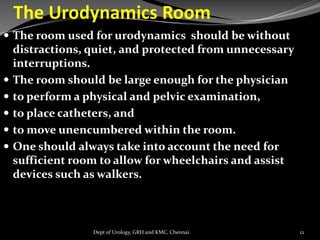
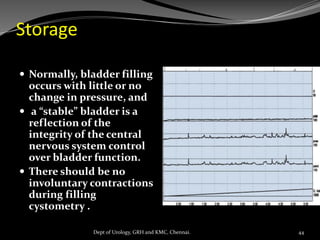
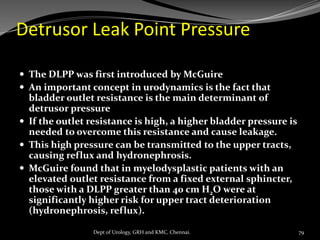
![Pitfalls in Cystometry
i. pressure measurement artifacts (the presence of air bubbles,
kinked tubing, incorrect placement, migration of the pressure
catheters) and
ii. infusion rate artifacts (especially in neurogenic bladder) and
iii. patient-related issues, including lack of cooperation, outlet
incompetence, and vesicoureteral reflux.
iv. If bladder filling is too rapid,
v. If the bladder outlet is incompetent, urine may leak around the
filling catheter and a low bladder compliance may not be
diagnosed because the bladder is never adequately filled (e.g.,
spinal dysraphism, severe intrinsic sphincter deficiency [ISD] in
an older woman).
47
Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/uds-voidingdysfunction-converted-210616031620/85/URODYNAMIC-EVALUATION-47-320.jpg)
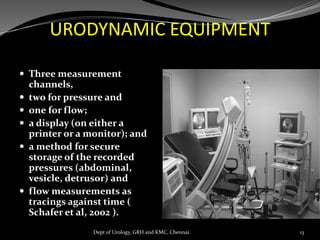
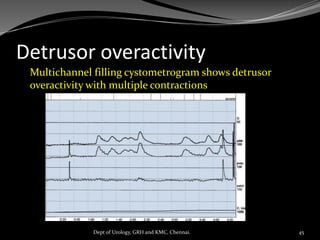
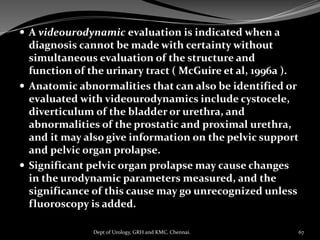
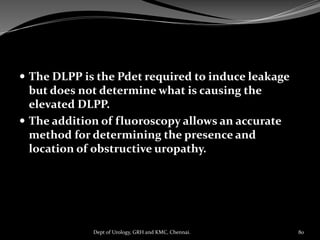
![ An index of bladder contractility (bladder
contractility index [BCI]) can be factored
PdetQmax + 5Qmax.
Using this formula for the BCI (i.e., BCI =
PdetQmax + 5Qmax),
BCI greater than 150 is strong,
BCI less than 100 is weak, and
BCI of 100 to 150 is normal
contractility .
63
Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/uds-voidingdysfunction-converted-210616031620/85/URODYNAMIC-EVALUATION-63-320.jpg)
























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)