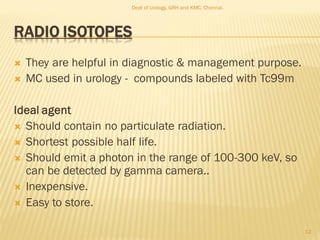
This document discusses the role of radioisotopes in urological diagnosis and management. It provides background on the history of radioisotopes and cyclotrons. It describes common radioisotopes used in urology like technetium-99m, iodine-131, gallium-67 and indium-111. The document discusses how different radioisotopes can be used to image renal function and structure, renal infections, and urological cancers like kidney cancer, bladder cancer and prostate cancer. Key applications of different radioisotopes are summarized.






![Current and new agents undergoing clinical study for radionuclide
imaging of PCainclude:
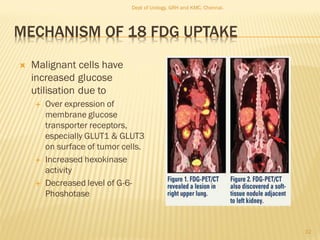
2-18F-fluoro-2-deoxy-D-glucose (FDG)
111In-7E11 antibody(ProstaScint™)
18F-fluorodihydrotestosterone (18F-FDHT)
radioacetateanalogs
radiocholine analogs
anti-1-amino-3-18Ffluorocyclobutane-1-carboxylic acid(anti-
[18F]FACBC)
37
Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/radioisotopesinurology-210614083421/85/Radioisotopes-in-urology-37-320.jpg)



![RADIONEUCLIDE CYSTOGRAM
Sensitive in detecting reflux
Significant lower absorbed
radiation
Use
1. Follow up of documented
reflux
2. Screening siblings of children
with reflux
Agents–DTPA, sulfur colloid,
pertechnate [ preferred],
MAG3
48
Dept of Urology, GRH and KMC, Chennai.](https://image.slidesharecdn.com/radioisotopesinurology-210614083421/85/Radioisotopes-in-urology-48-320.jpg)















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)








