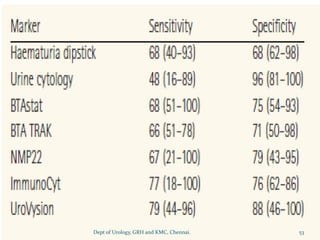
This document provides information about various tumor markers used in urology, including prostate-specific antigen (PSA) markers for prostate cancer screening and diagnosis, tumor markers for testicular cancer such as alpha-fetoprotein (AFP) and human chorionic gonadotropin (HCG), and urine-based markers for bladder cancer screening like NMP22 and BTA. It also discusses guidelines for PSA screening and interpretation, as well as clinical applications of different tumor markers for diagnosis, prognosis, monitoring treatment response, and detecting recurrence of urological cancers.












































![Enzyme_Tumour_Markers[1] [Read-Only].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/enzymetumourmarkers1read-only-260123213318-97319479-thumbnail.jpg?width=640&height=640&fit=bounds)

































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









