Downloaded 44 times
























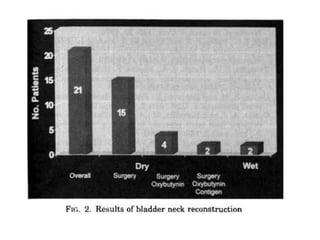
























This document discusses various surgical procedures for bladder neck reconstruction to treat neurogenic bladder dysfunction. It describes several techniques such as flap valve mechanisms, bulking agents, and artificial urinary sphincters that aim to tighten the bladder neck. No single procedure is best for all patients and options must be tailored based on each person's condition and goals. While many techniques have shown success rates over 90% for continence, factors like learning curves, variable definitions of success, and prior reconstruction attempts can influence outcomes. Complications include incontinence, fistulas, and tissue necrosis, so careful patient selection and follow-up is important.