Downloaded 137 times



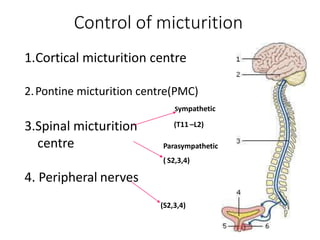


































This document provides an overview of neurogenic bladder including: 1. Neurogenic bladder affects 15% of the population and symptoms increase with age. Bladder dysfunction can negatively impact quality of life. 2. The bladder has storage and voiding functions controlled by the brain and spinal cord. Detrusor overactivity, detrusor-sphincter dyssynergia, and detrusor areflexia are types of neurogenic bladder dysfunction. 3. Investigations include post-void residual volume, uroflowmetry, and cystometry to evaluate the bladder and determine appropriate treatment which may include anticholinergics, botulinum toxin injections, clean intermittent catheterization, or surgery


































![Neurogenic bladder [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/neurogenicbladderedmond-140716213757-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)














































