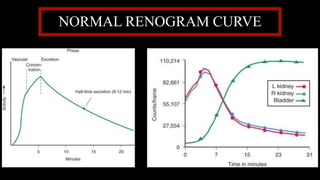
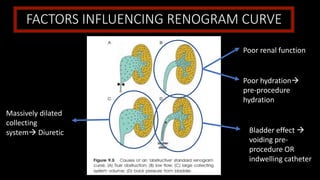
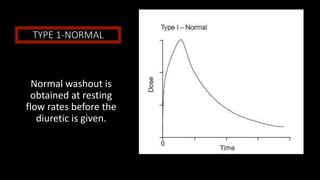
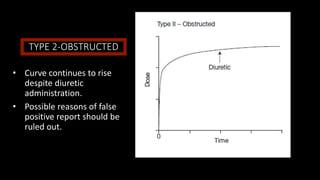
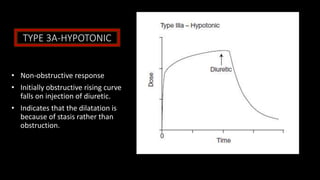
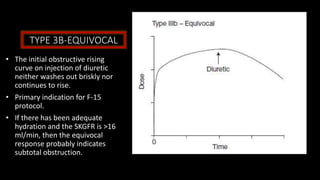
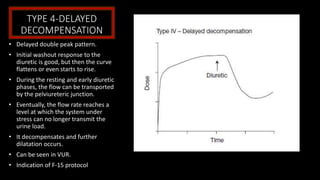
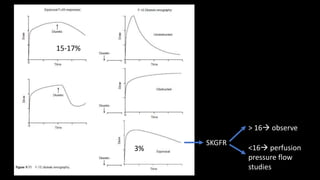
This document discusses diuresis renography, a technique used to differentiate patients with equivocal obstruction of the upper urinary tract. It involves injecting a patient with a radiopharmaceutical and obtaining images as a diuretic is administered. The resulting renogram curves are analyzed to identify four potential curve patterns: normal washout indicating no obstruction; continued rise indicating obstruction; initial rise falling with diuresis indicating hypotonicity rather than obstruction; and delayed decompensation indicating subtotal obstruction. Using different timing protocols for diuretic administration, such as F-15 where it is given 15 minutes before imaging, can reduce equivocal results from 15-17% to 3%.