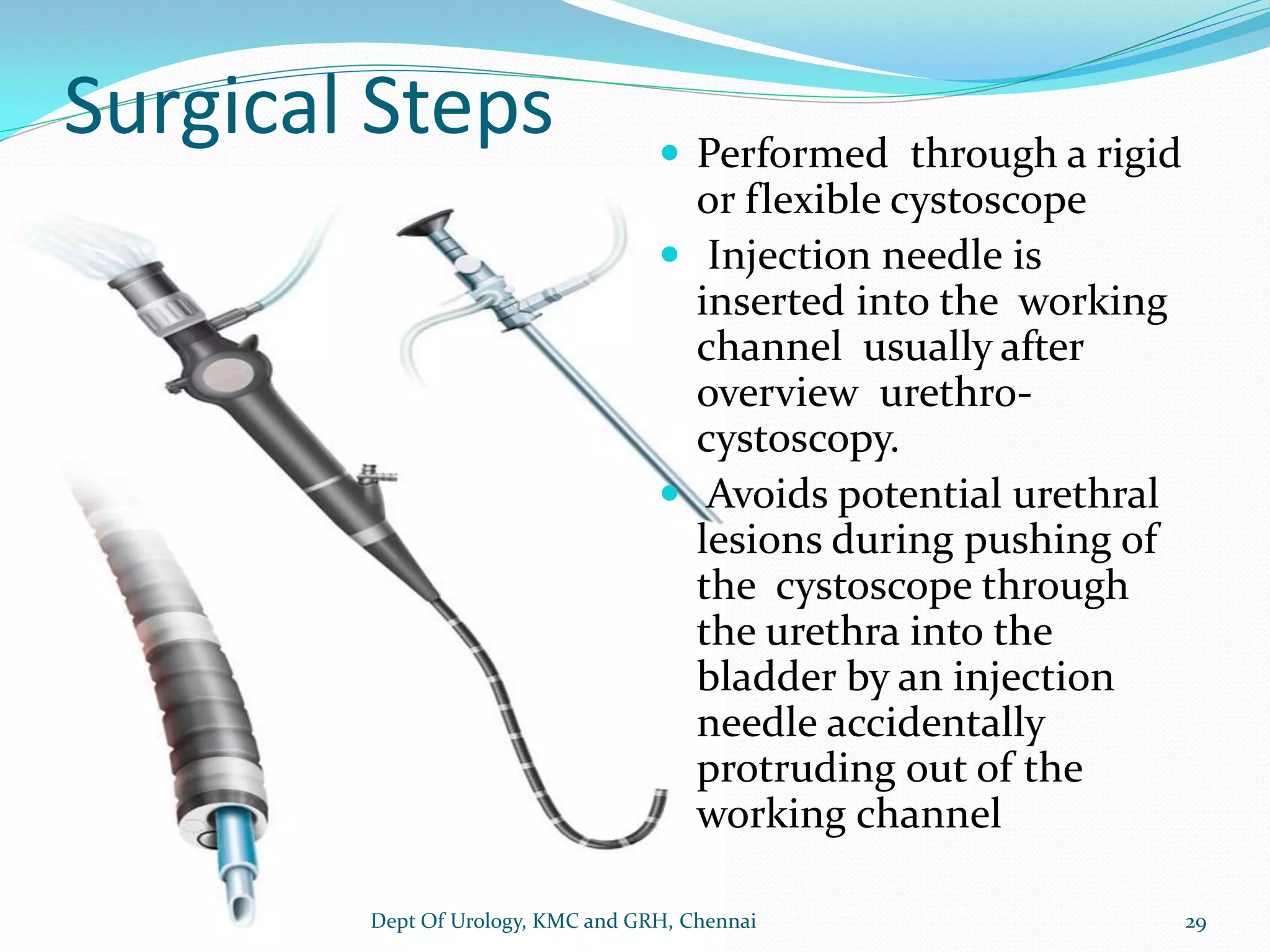
This document provides information about botulinum toxin including its mechanism of action, uses in urology, administration techniques, and outcomes. It discusses how botulinum toxin works by inhibiting acetylcholine release at nerve terminals, preventing muscle contraction. It is used to treat overactive bladder, detrusor overactivity, and other urologic conditions by injecting the toxin into the bladder or sphincter under cystoscopic guidance. When administered properly, botulinum toxin significantly improves urinary symptoms and quality of life for several months.