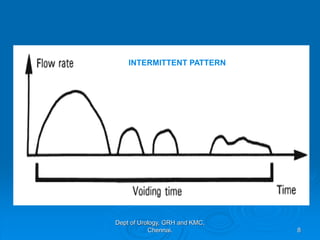
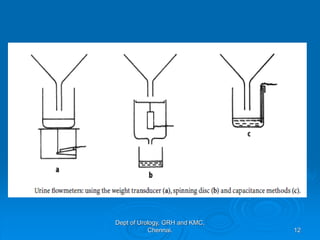
This document describes uroflowmetry - a noninvasive test used to evaluate urine flow. It discusses the normal and abnormal flow patterns seen in uroflowmetry and their clinical significance. Uroflowmetry provides parameters like maximum flow rate, average flow rate and voided volume. It can detect bladder outlet obstruction, detrusor underactivity or overactivity. However, pressure-flow studies are needed to precisely define lower urinary tract function. Uroflowmetry is useful for screening and monitoring treatment response, though invasive therapy should not be based on uroflowmetry alone per AUA guidelines.