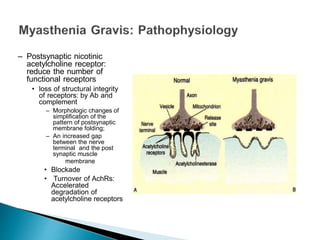
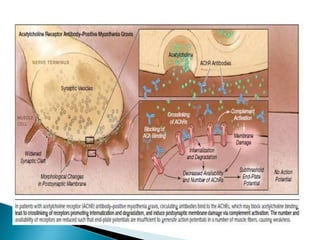
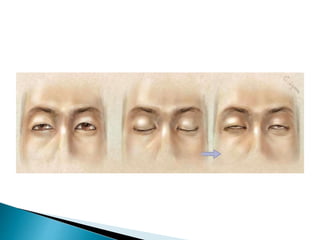
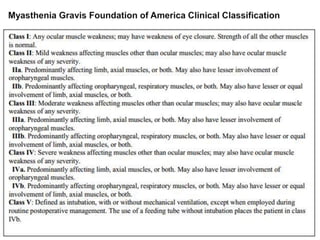
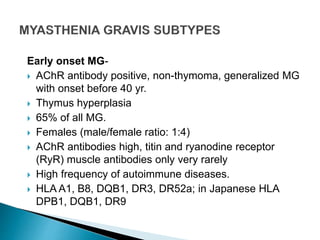
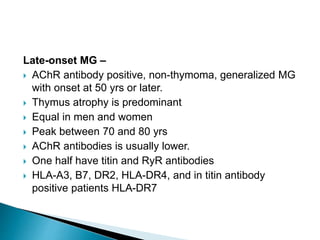
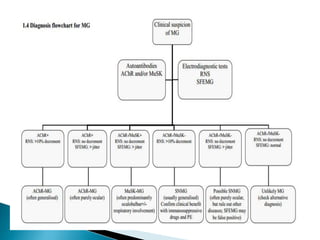
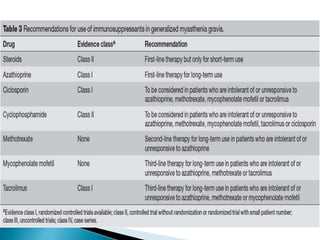
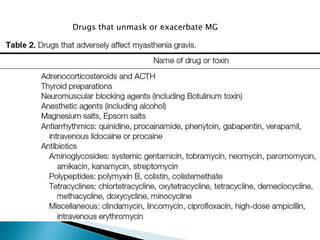
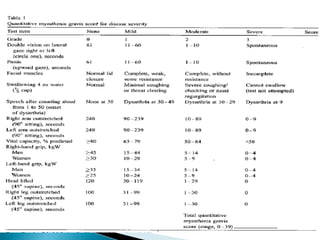
This document provides information on Myasthenia Gravis (MG), an autoimmune neuromuscular disease caused by antibodies against postsynaptic muscle membranes. It discusses the prevalence and classification of MG, clinical features including weakness and fatigability, diagnostic testing such as repetitive nerve stimulation and edrophonium testing, treatment including acetylcholinesterase inhibitors and immunotherapies, and management of symptoms. Key points covered include the fluctuating muscle weakness that worsens with exertion seen in MG, different classifications based on symptoms and severity, and first line treatment involving pyridostigmine and corticosteroids.









































































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)



































