Downloaded 205 times


Myasthenia Gravis is an autoimmune neuromuscular disorder characterized by weakness of skeletal muscles that worsens with exertion and improves with rest. It results from antibodies directed against acetylcholine receptors at the neuromuscular junction, reducing their numbers and impairing signal transmission from nerves to muscles. Diagnosis involves testing for antibodies, electrodiagnostic studies like repetitive nerve stimulation and single fiber EMG, and response to medications like edrophonium. Treatment focuses on acetylcholinesterase inhibitors, immunomodulators like corticosteroids, plasmapheresis, and thymectomy in cases involving thymoma.
Introduction to Myasthenia Gravis (MG) and its outline including background, anatomy, and treatment.
Acquired autoimmune disorder characterized by skeletal muscle weakness and fatigability, first described in 1672.
Details on the structure of the neuromuscular junction (NMJ) including components and functions of acetylcholine and its receptors.
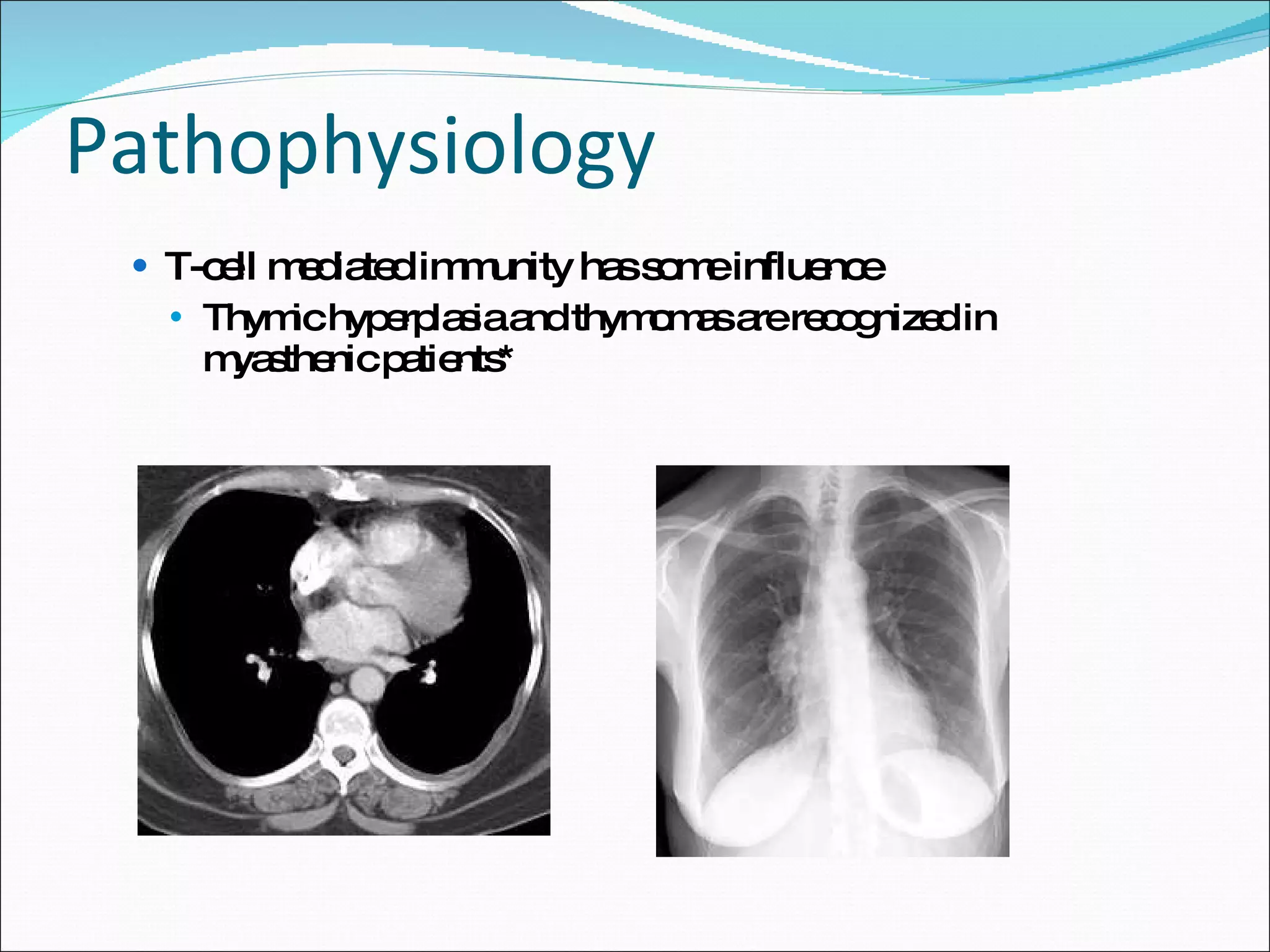
Antibody response at the NMJ in MG leading to receptor loss and potential B cell involvement, including thymic factors.
Frequency and risk factors of MG, including incidence in the US (2/1,000,000) and worldwide prevalence (1/10,000).
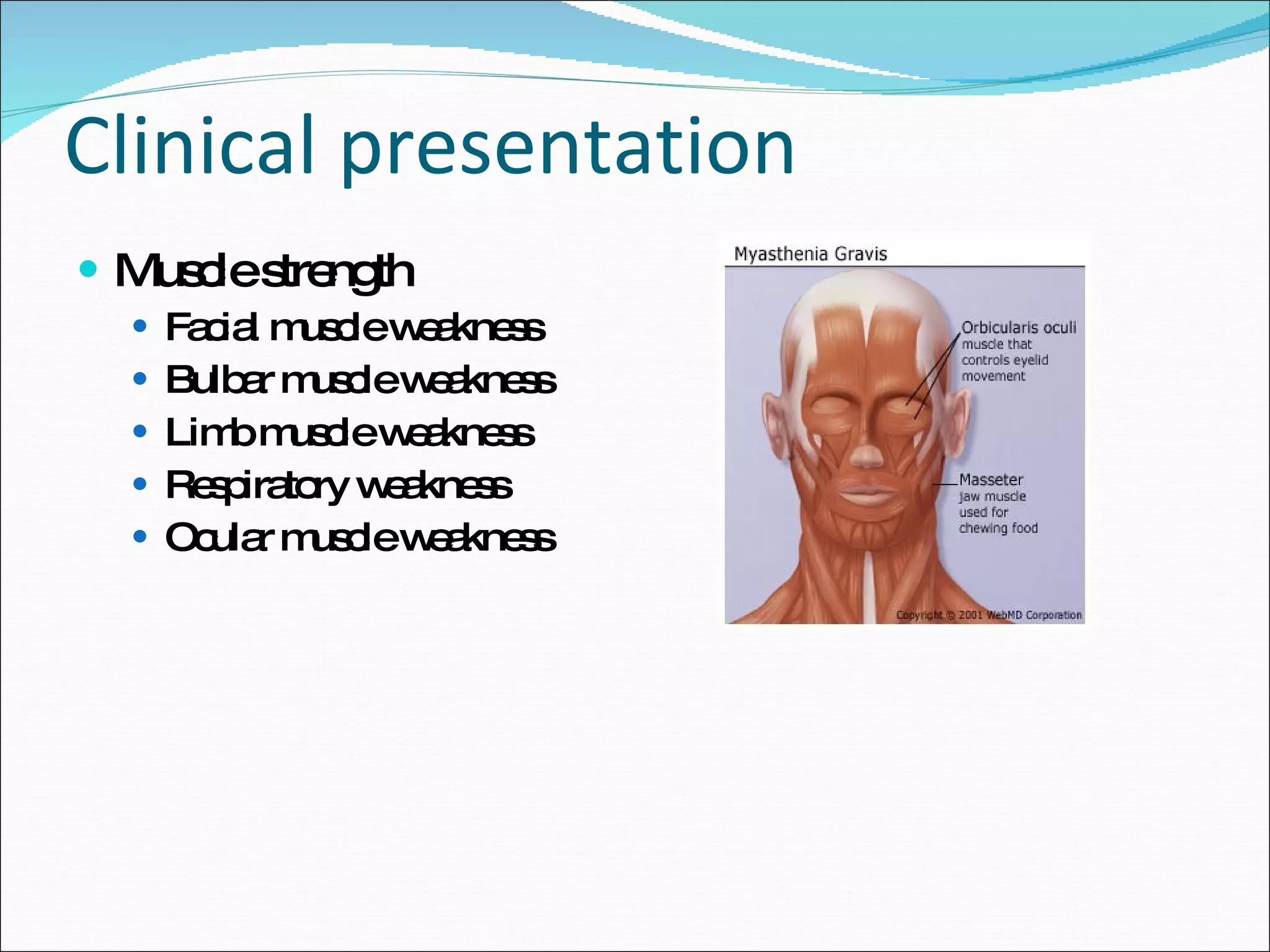
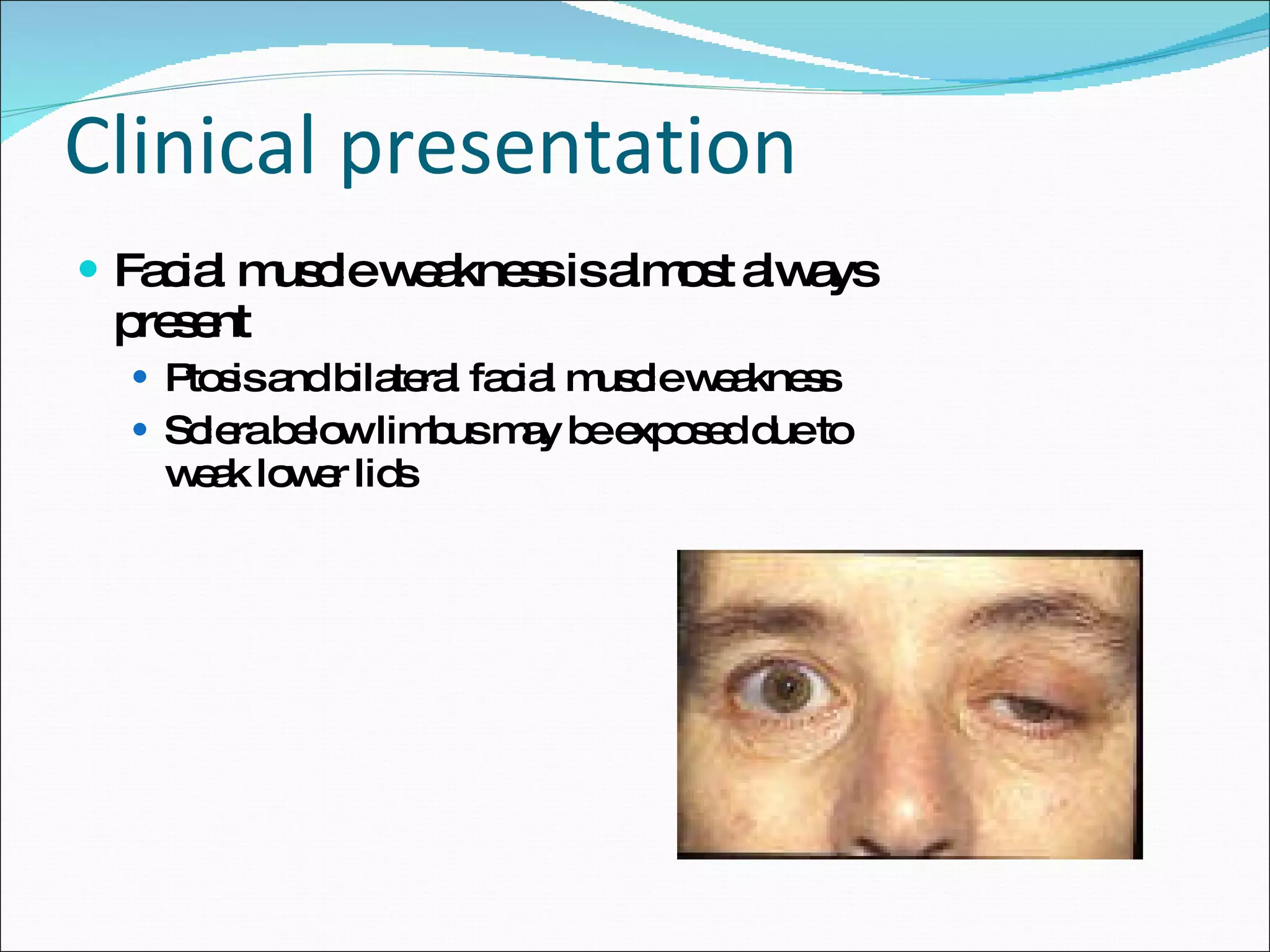
Fluctuating muscle weakness, ocular symptoms, bulbar, and limb weakness; associated autoimmune conditions.
List of conditions to differentiate from Myasthenia Gravis including ALS, multiple sclerosis, and others.
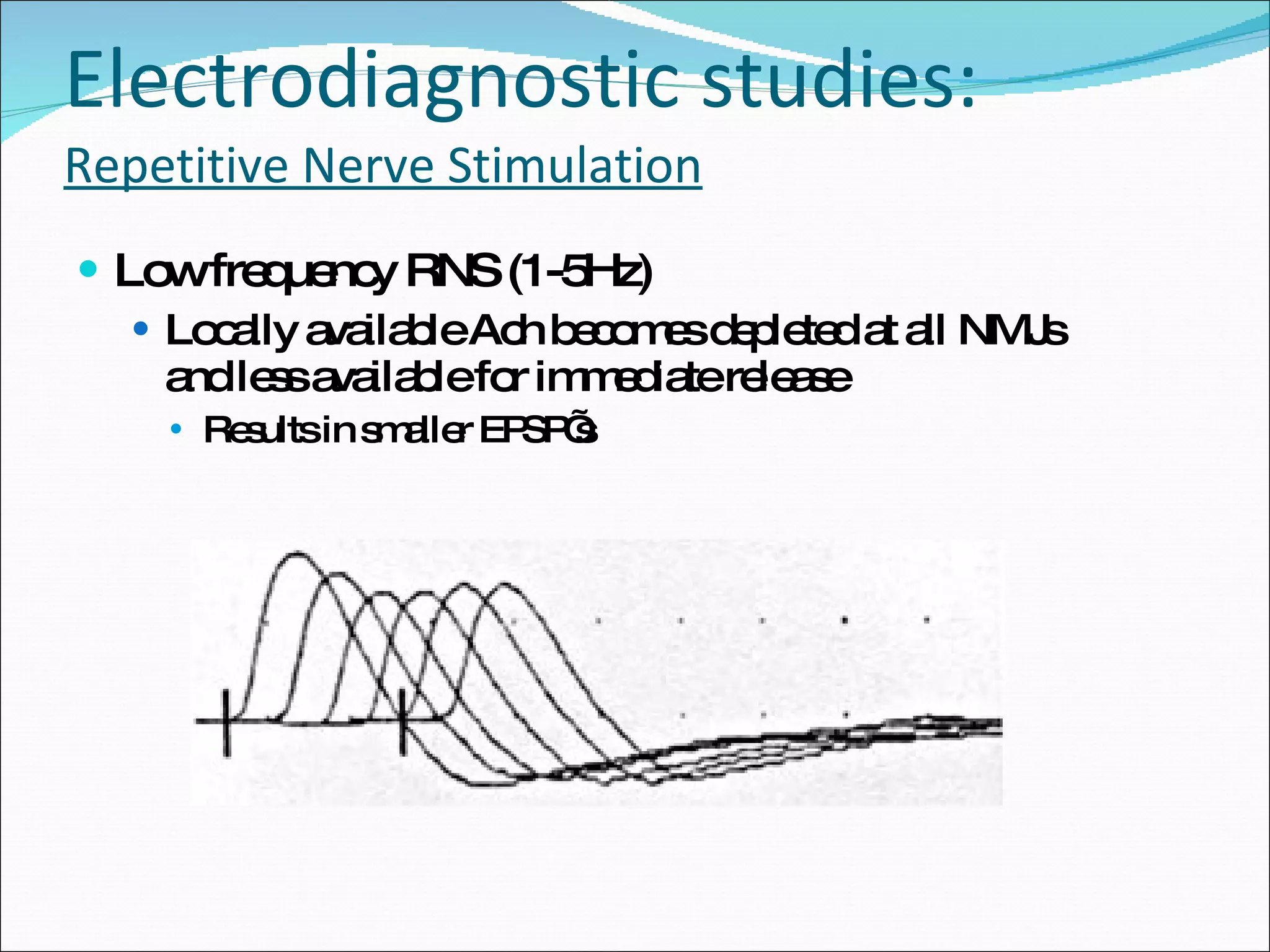
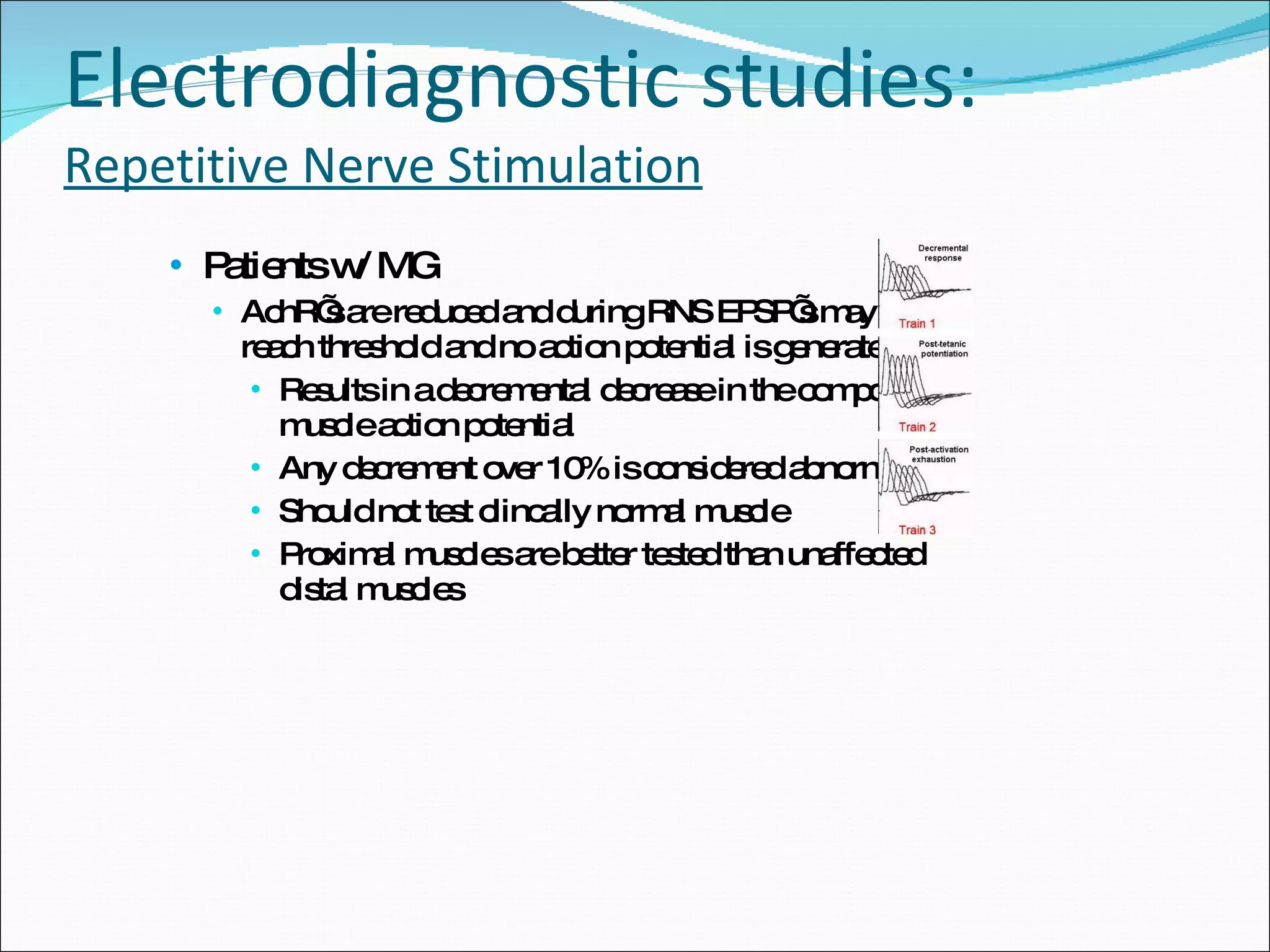
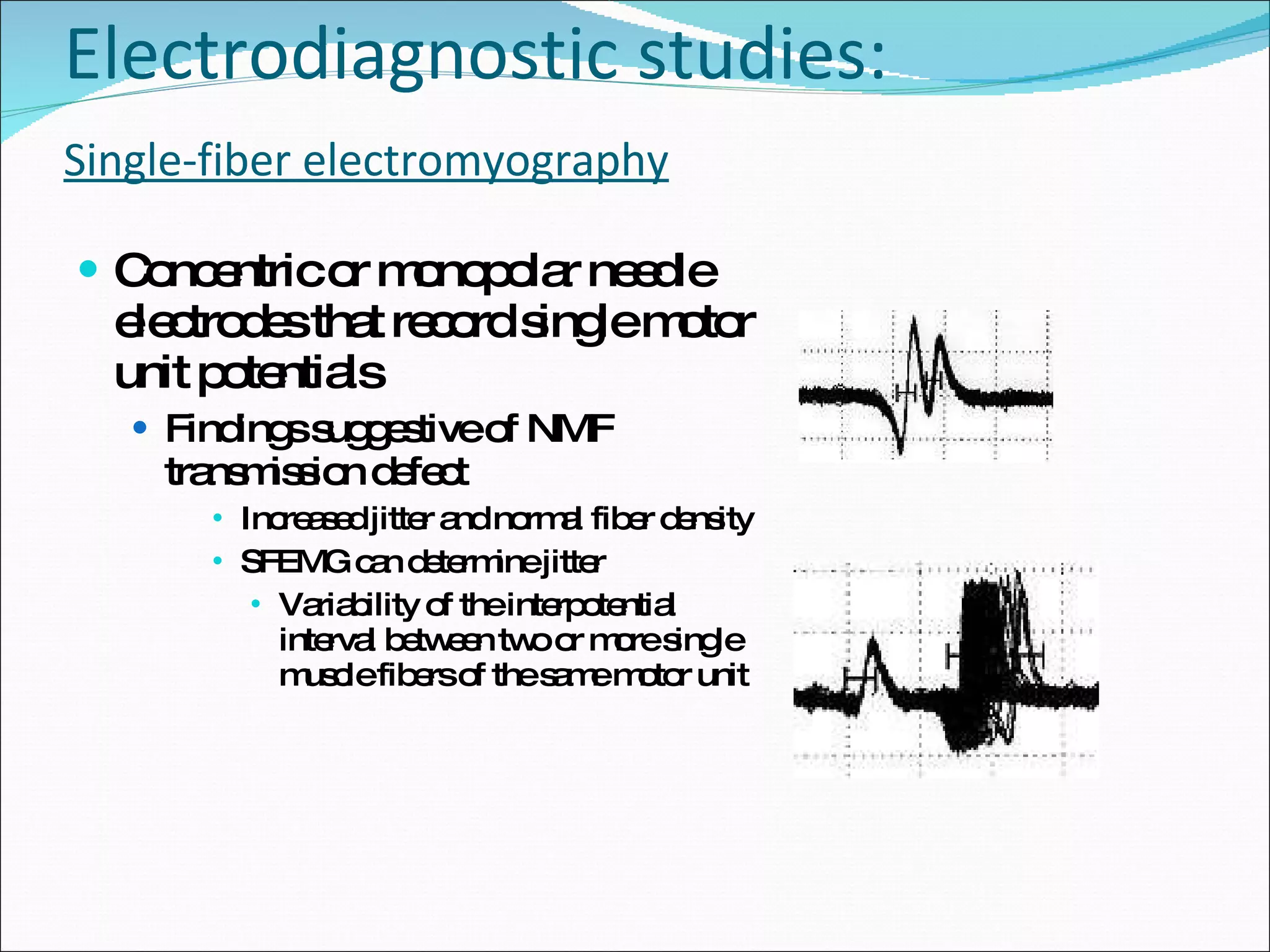
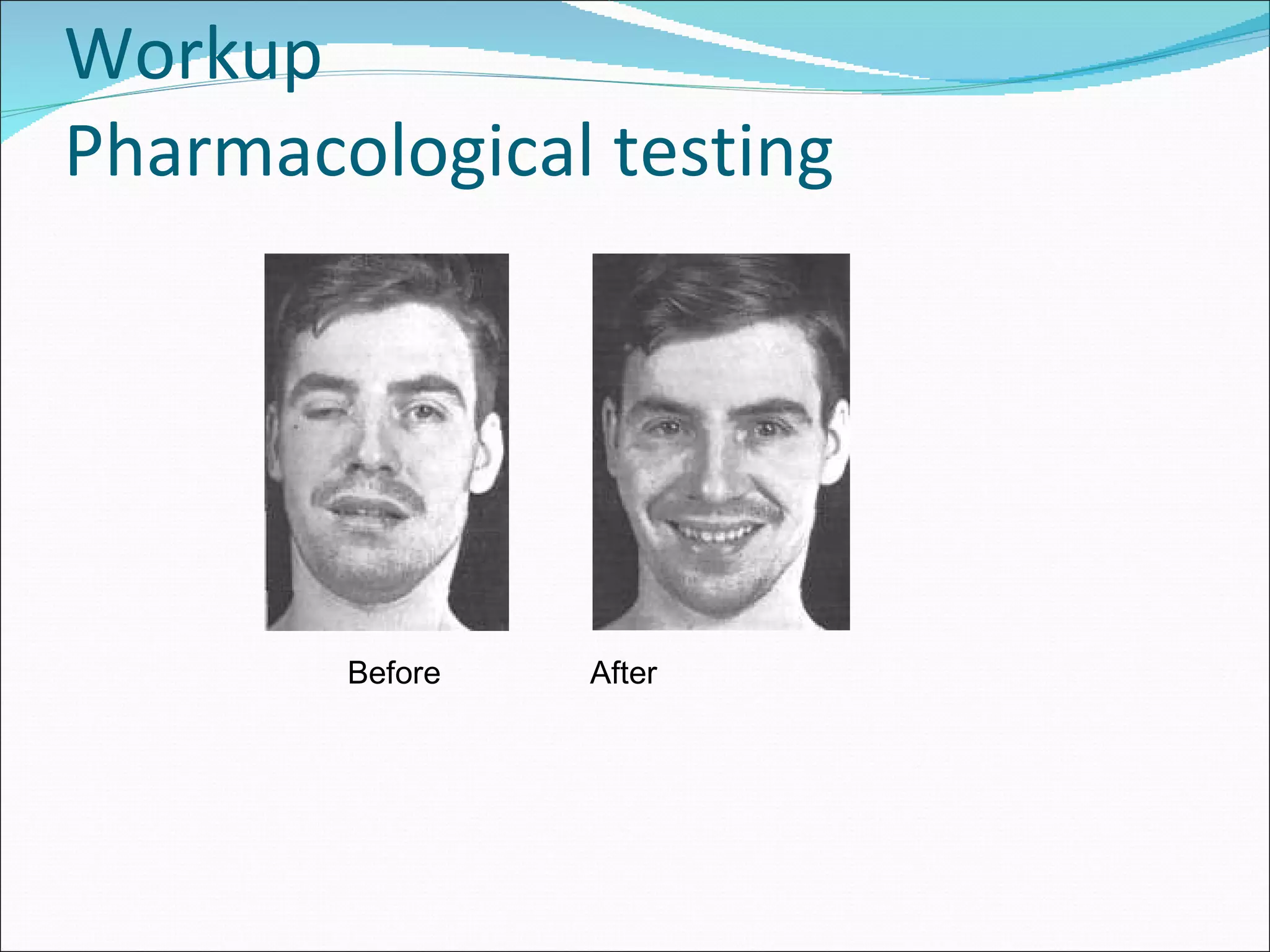
Laboratory tests, imaging studies, electrodiagnostic studies, and pharmacological testing to confirm MG.
Therapies including AChE inhibitors, immunomodulating therapies, dietary modifications, and management of complications.
Mortality statistics and rehabilitation strategies focusing on patient education and adaptive support.
Cited literature and sources for further reading on Myasthenia Gravis.









































































































