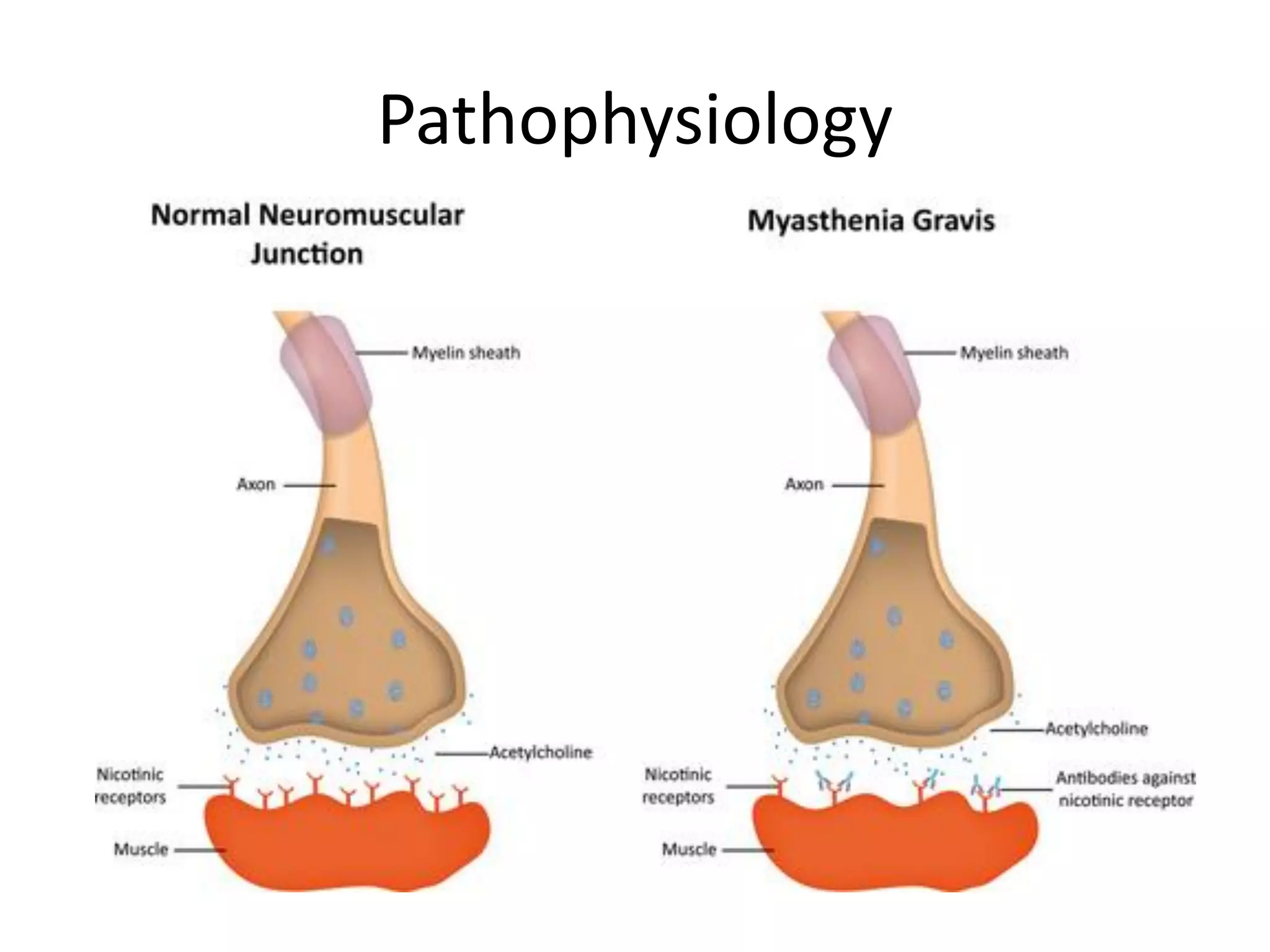
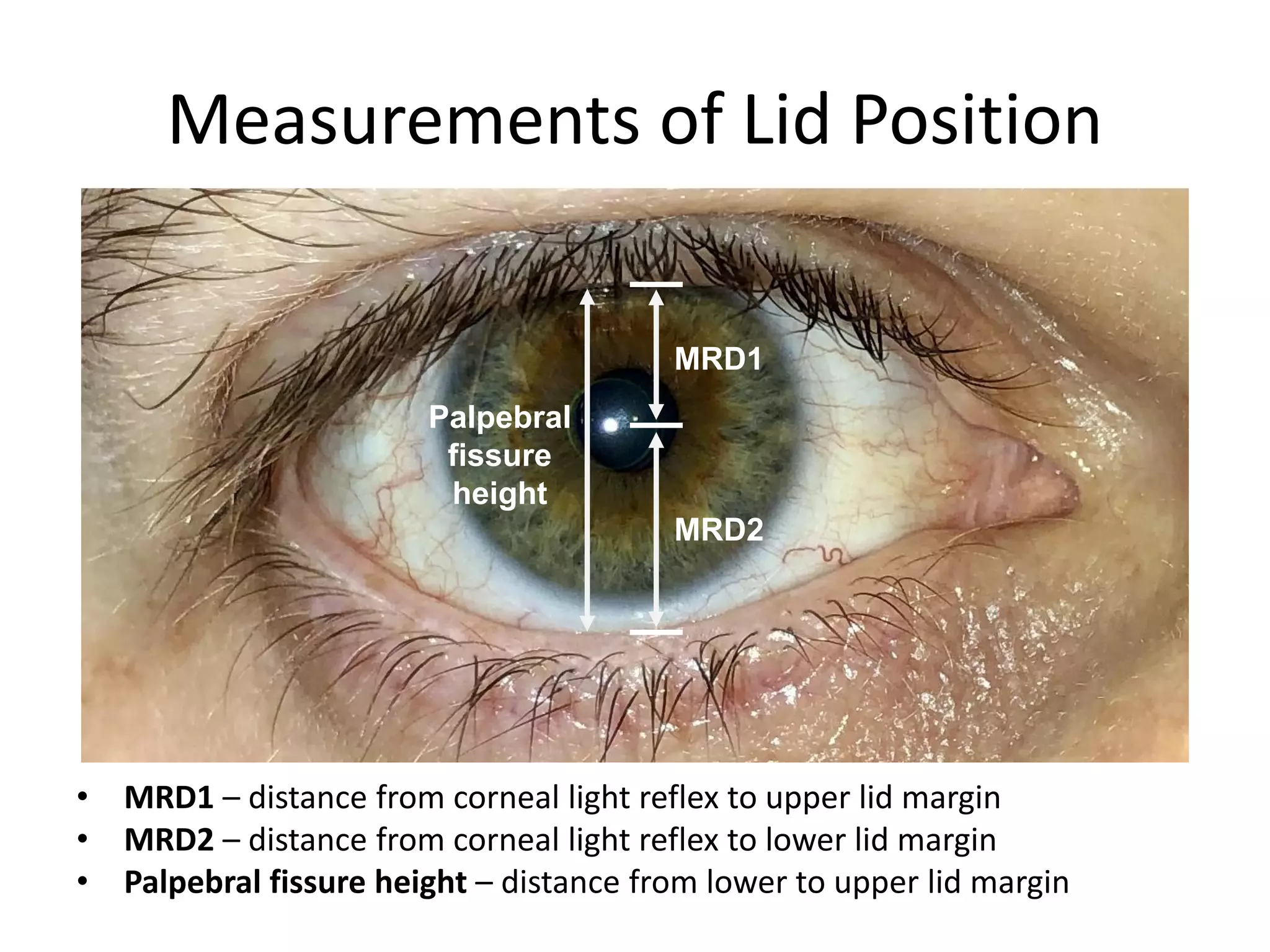
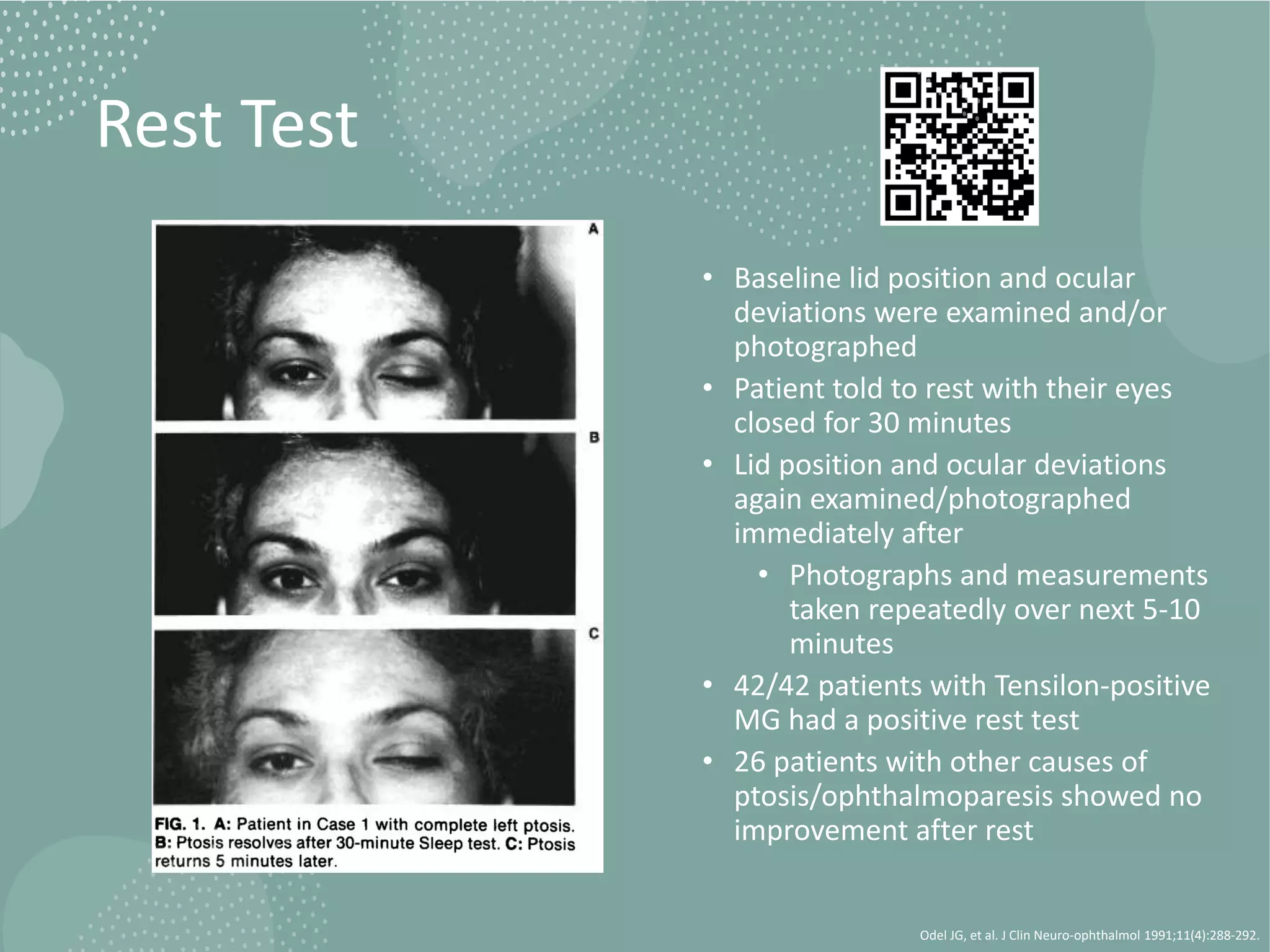
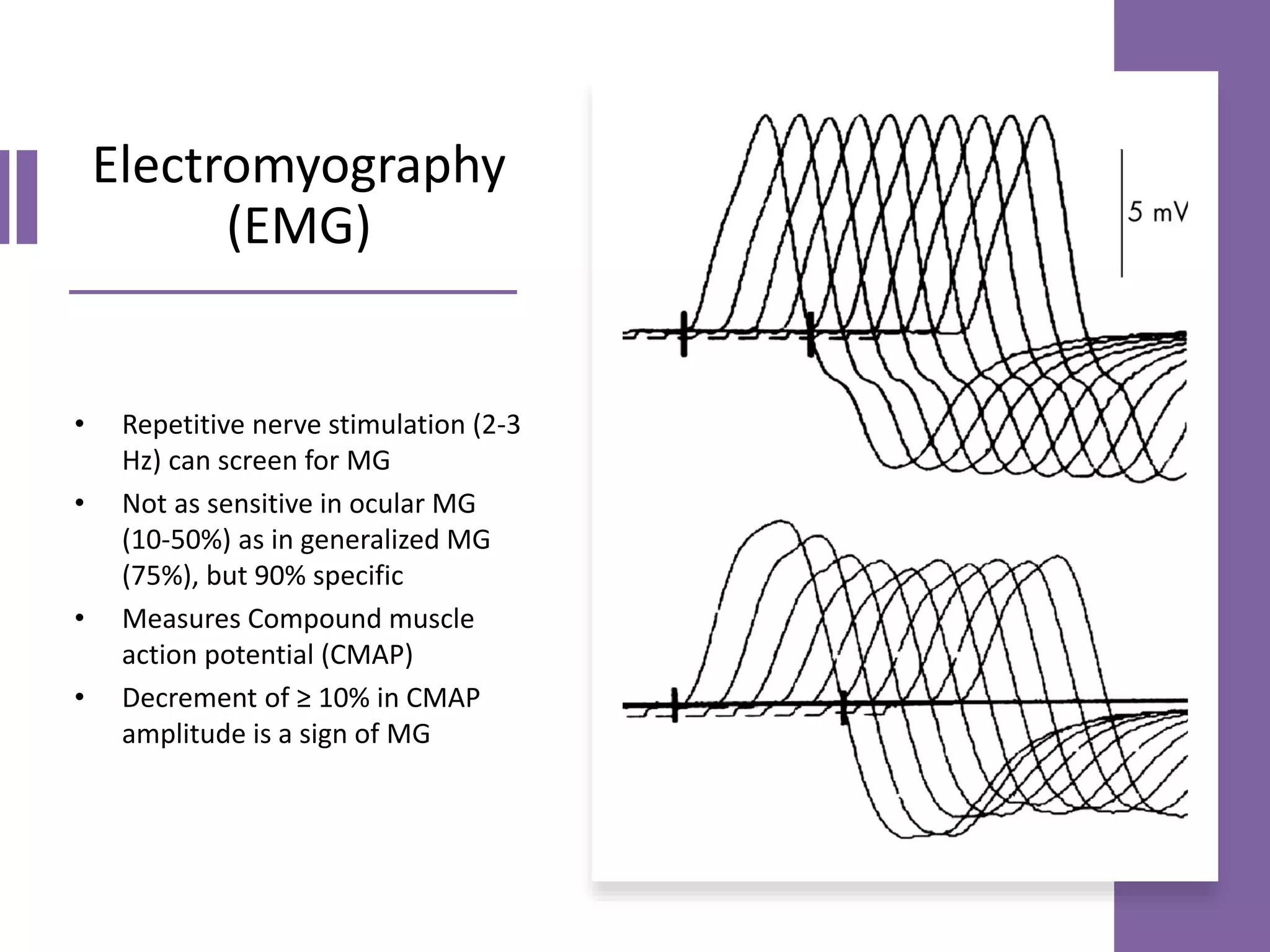
This document provides an overview of ocular myasthenia gravis (OMG), including pathophysiology, clinical presentation, diagnostic testing, and management. Key points include: OMG is caused by antibodies impairing acetylcholine receptors, causing muscle weakness that worsens with use. Common symptoms are fluctuating ptosis and diplopia. Diagnosis involves history, exam findings like fatigable ptosis, and may include tests like ice pack, Tensilon/neostigmine, EMG. Treatment focuses on pyridostigmine and immunosuppression with prednisone and azathioprine. Thymectomy may be considered for generalized cases under age 50.





















































![Myasthenia gravis guest_lecture[1]](https://cdn.slidesharecdn.com/ss_thumbnails/myastheniagravisguestlecture1-120720130546-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)

























































