Downloaded 381 times
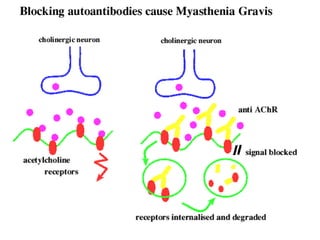
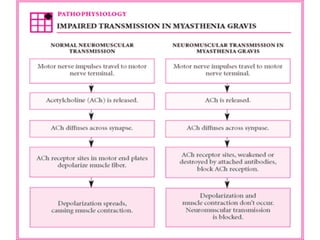


Myasthenia gravis is an autoimmune disorder characterized by varying degrees of weakness of voluntary muscles. It is caused by antibodies against acetylcholine receptors at the neuromuscular junction, impairing transmission of nerve impulses to muscles. Symptoms include drooping eyelids, double vision, weakness of facial muscles and difficulty swallowing. It occurs most commonly in young adult women and older men. While its cause is unknown, treatment involves anticholinesterase drugs, immunosuppressants, plasmapheresis, IVIG, and sometimes thymectomy. Complications include myasthenic crisis with severe generalized weakness and respiratory failure.











































































































