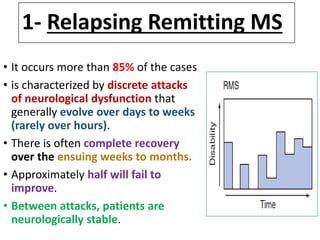
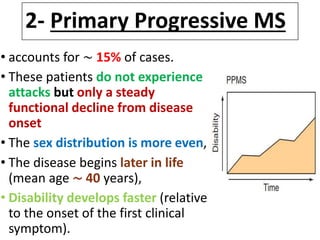
Multiple sclerosis is a chronic disease characterized by inflammation, demyelination, and gliosis in the central nervous system. It affects around 5 million people worldwide. The cause is unknown but involves genetic and environmental factors. Symptoms vary widely and can include sensory disturbances, motor symptoms, visual problems, ataxia, and cognitive impairment. Diagnosis involves demonstrating dissemination of lesions in the CNS over time via MRI imaging or evoked potentials testing, and sometimes analysis of cerebrospinal fluid. There are several disease courses including relapsing-remitting MS, primary progressive MS, and secondary progressive MS. Management aims to reduce inflammation and disability progression.



























































![Multiple sclerosis- Sushila [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/multiplesclerosis-sushilaautosaved-230522133935-4f68df92-thumbnail.jpg?width=640&height=640&fit=bounds)