This document provides information about Myasthenia Gravis (MG), including its epidemiology, clinical presentation, immunopathology, diagnostic procedures, treatment, and management of different subtypes. Some key points include:
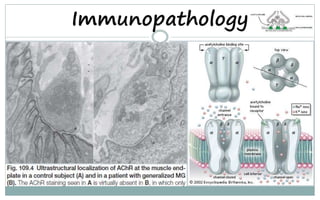
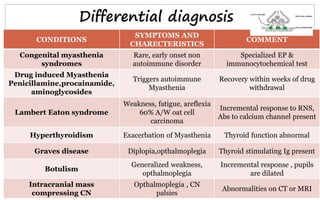
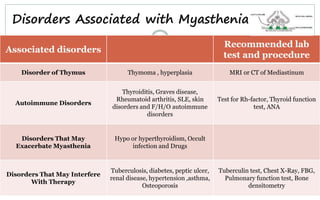
- MG is an autoimmune disorder causing muscle weakness due to antibodies interfering with acetylcholine receptors at the neuromuscular junction.
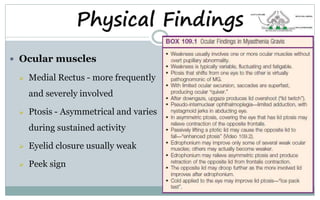
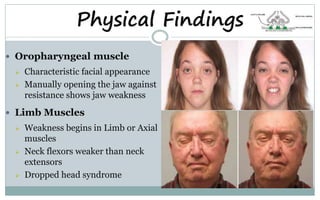
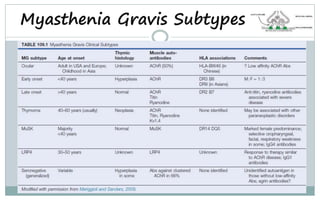
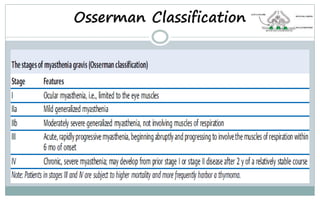
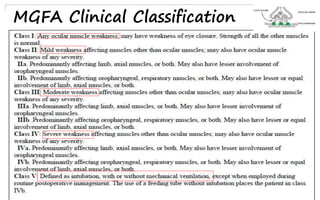
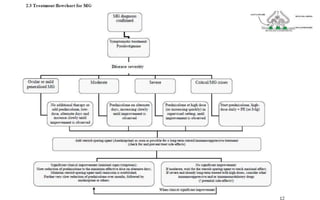
- It can present with symptoms like ptosis, diplopia, limb or swallowing weakness.
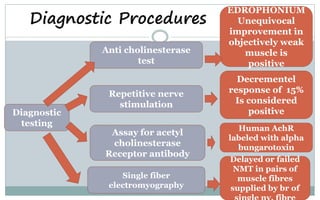
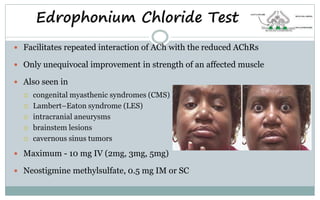
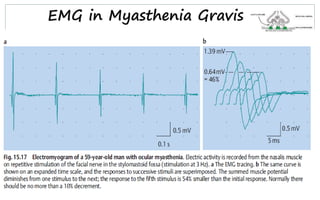
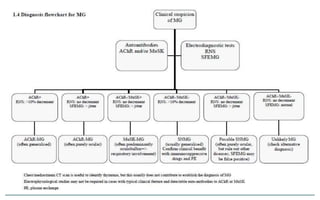
- Diagnosis involves tests like repetitive nerve stimulation, serum acetylcholine receptor antibody levels, and single fiber electromyography.
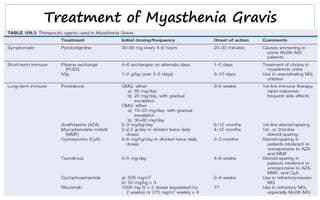
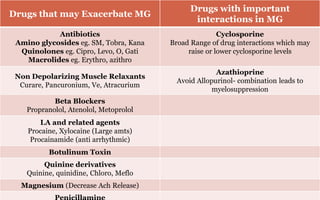
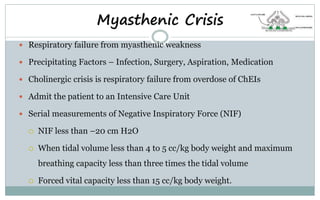
- Treatment includes pyridostigmine, corticosteroids, immunosuppressants, IVIG, plasma exchange,















![Myasthenia gravis guest_lecture[1]](https://cdn.slidesharecdn.com/ss_thumbnails/myastheniagravisguestlecture1-120720130546-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)










![Myelin Oligodendrocyte Glycoprotein (MOG) Antibody Disease [MOG-AD]](https://cdn.slidesharecdn.com/ss_thumbnails/myelinoligodendrocyteglycoproteinmogantibodydisease0920-200920055159-thumbnail.jpg?width=640&height=640&fit=bounds)

































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















