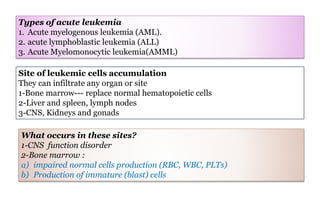
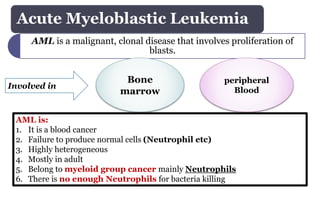
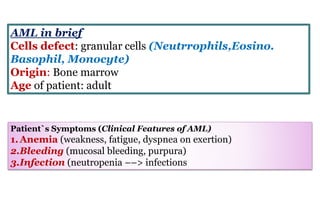
1. Acute myeloblastic leukemia (AML) is a cancer that involves the rapid growth of abnormal white blood cells that build up in the bone marrow and interfere with normal blood cell production.
2. It is the most common type of acute leukemia in adults. The leukemia cells are unable to effectively fight infections due to a lack of normal white blood cells.
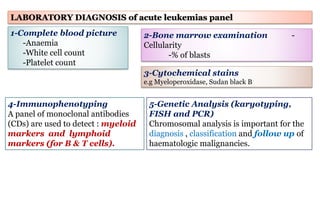
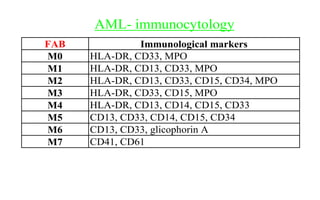
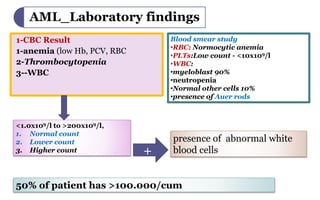
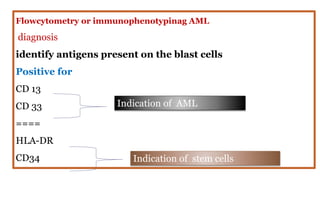
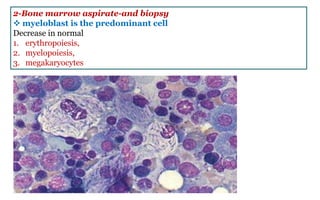
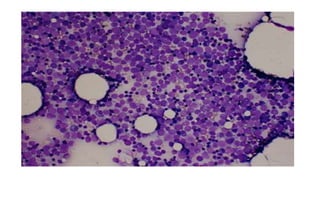
3. Diagnosis involves blood tests, bone marrow aspiration and biopsy, immunophenotyping via flow cytometry to identify cell antigens, and cytogenetic analysis to identify chromosomal abnormalities.






















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

