This document discusses hepatoblastoma (HB), a rare type of liver cancer that primarily affects young children. It provides details on:
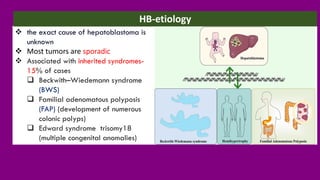
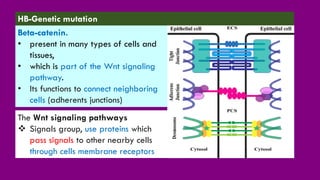
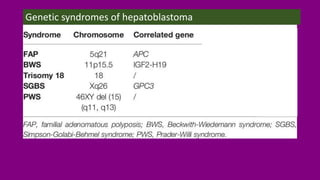
- The causes of HB including genetic mutations and syndromes.
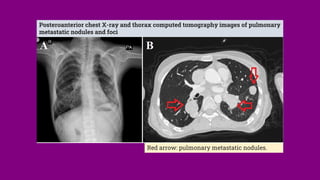
- Presenting symptoms like abdominal swelling and jaundice.
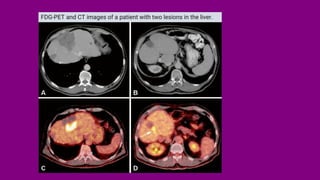
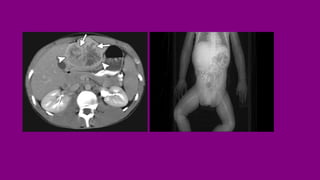
- Diagnosis involving blood tests, imaging like CT/MRI, and biopsy.
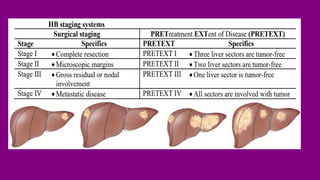
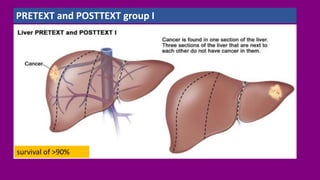
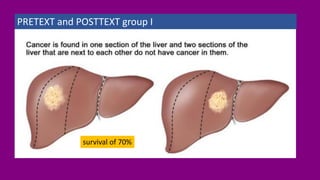
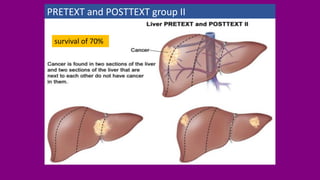
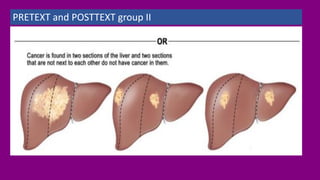
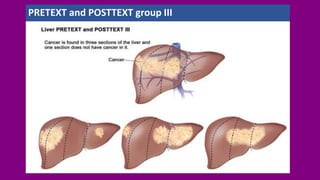
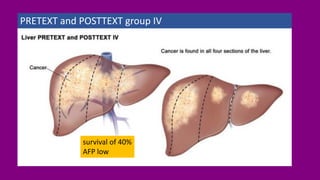
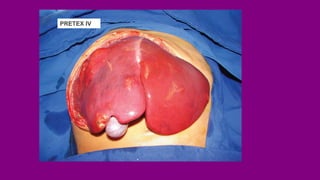
- Staging HB using the PRETEXT and POSTTEXT systems to determine if the tumor can be surgically removed.
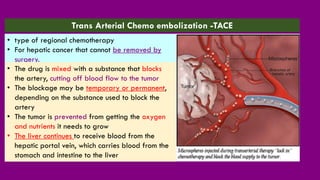
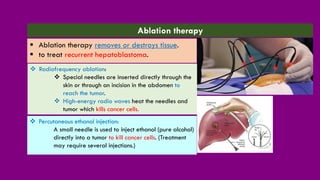
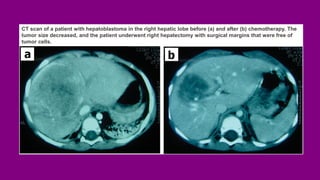
- Treatment options including chemotherapy, radiation, surgery, and targeted therapy.
- Prognosis factors like age, tumor markers, and response to initial treatment.