The document discusses chronic lymphocytic leukemia (CLL), including its definition, epidemiology, etiology, pathogenesis, clinical symptoms, diagnosis, staging, prognosis, and treatment. Some key points:
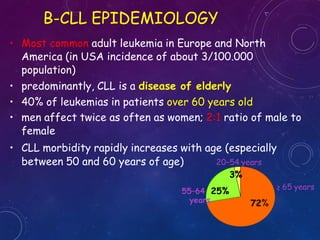
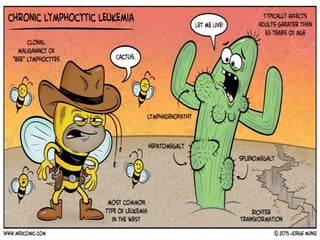
- CLL is characterized by the proliferation and accumulation of small, mature lymphocytes in the blood, bone marrow, and lymphoid tissues. It most commonly affects elderly adults.
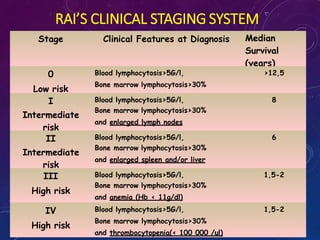
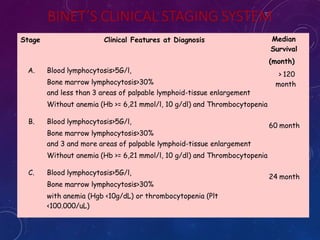
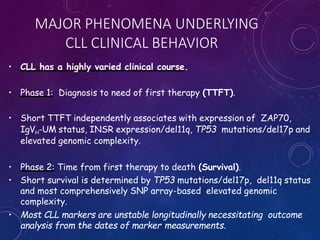
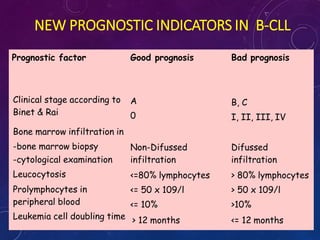
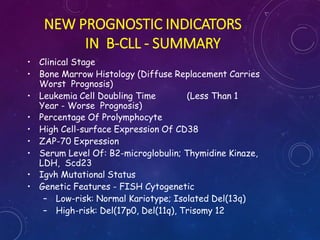
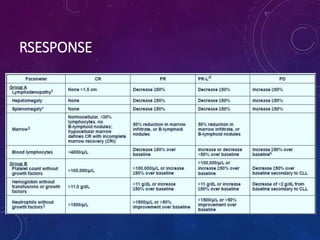
- Diagnosis is based on blood cell counts and immunophenotyping of lymphocytes. Prognosis depends on factors like clinical stage, genomic abnormalities, and biomarker expression levels.
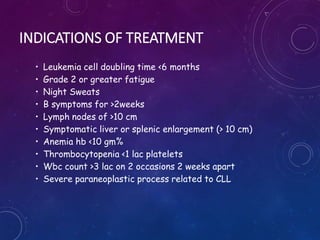
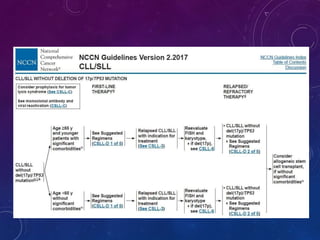
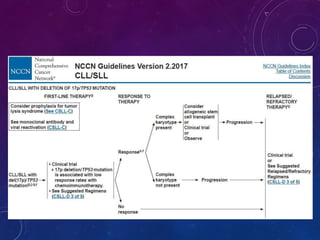
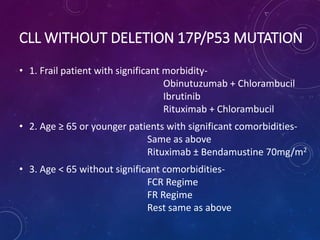
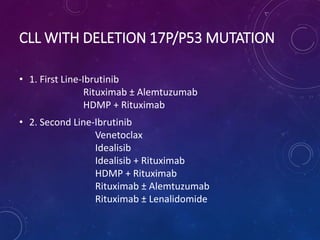
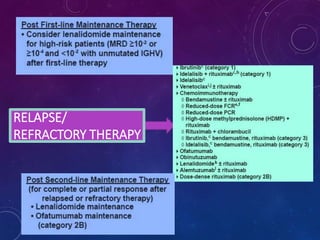
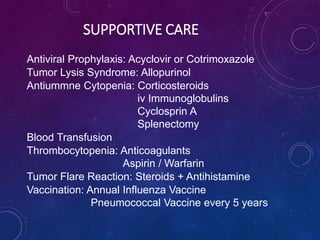
- Treatment involves chemotherapy, chemoimmunotherapy, targeted therapies, and supportive care. The appropriate treatment approach depends on a patient's risk




























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)