Downloaded 99 times

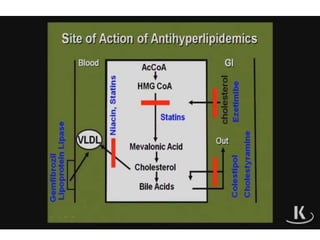

Hyperlipidemia refers to elevated levels of lipids or lipoproteins in the blood. It is caused by disorders involving elevations of lipoproteins such as low-density lipoprotein (LDL), very low-density lipoprotein (VLDL), and triglycerides. This puts one at risk for complications like atherosclerosis and pancreatitis. Treatment involves medications that lower LDL and triglyceride levels such as statins, resins, fibrates, and nicotinic acid. Each work by different mechanisms but commonly decrease lipid synthesis or increase lipid clearance to normalize lipid profiles and reduce cardiovascular risk. Side effects depend on the specific drug but may include gastrointestinal issues or myopathy.




















































![Agents_Used_in__dyslipidemyryyyia[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/agentsusedindyslipidemia1-260115112511-ee52bd07-thumbnail.jpg?width=640&height=640&fit=bounds)










































