Downloaded 897 times


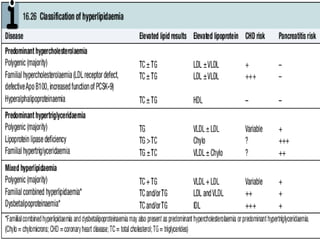
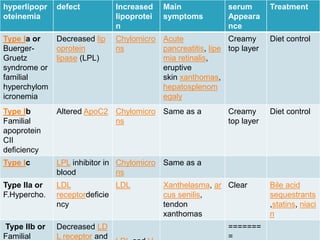
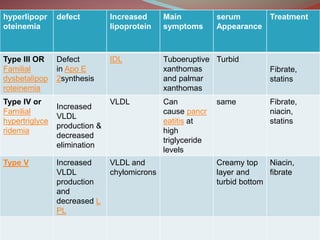

Hyperlipidemia involves abnormally elevated levels of lipids and lipoproteins in the blood. Lipids include cholesterol, triglycerides, and phospholipids, which are transported around the body within lipoproteins like chylomicrons, VLDL, LDL, IDL, and HDL. High cholesterol and triglycerides are major risk factors for cardiovascular disease, and very high triglycerides can cause pancreatitis. Hyperlipidemias can be primary or secondary, and are classified based on which lipids are predominantly elevated, such as cholesterol, triglycerides, or both. Primary causes include genetic defects or polygenic influences, while secondary causes include hypothyroidism, pregnancy, liver disease



































































