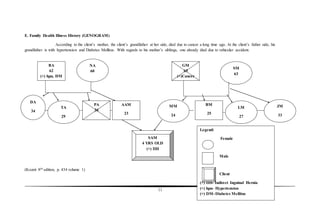
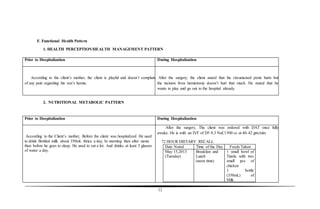
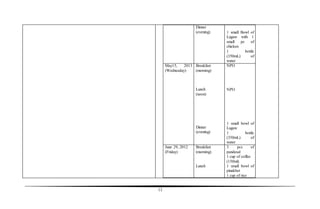
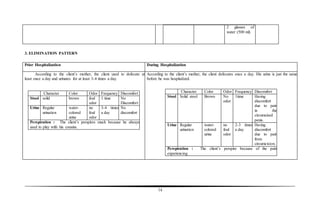
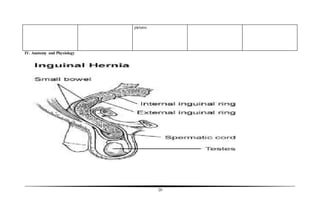
The document presents a case study of a 4-year-old boy diagnosed with an indirect inguinal hernia and undescended testes, highlighting the condition's medical implications, types of hernias, and nursing assessments. It details the patient's medical history, symptoms, treatment plan, and nursing care objectives, aiming to enhance understanding and management of this health issue amongst nursing students. Additionally, the study serves as a reference for future research on hernias in nursing education.