Downloaded 3,069 times

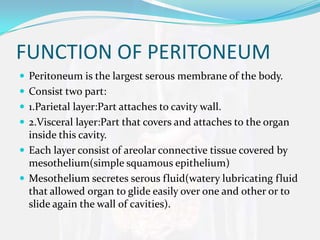

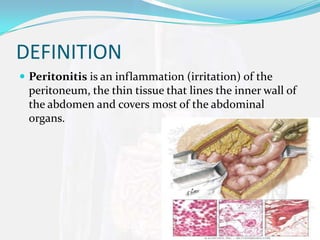






The peritoneum is a membrane that lines the abdominal wall and covers abdominal organs. It consists of parietal and visceral layers composed of mesothelium that secretes fluid allowing organs to glide. Peritonitis is inflammation of the peritoneum caused by infections from medical procedures, ruptured organs, or trauma which leads to abdominal pain and infection symptoms treated with antibiotics and sometimes surgery.























































































